| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
DYSPEPTIC PAIN
A newly recognized emergency thirst signal of the human body.
Dyspeptic pain is the most important signal for the human body. It denotes dehydration. It is a thirst signal of the body. It can occur in the very young, as well as in older people. Chronic and persistently increasing dehydration is the root cause of almost all currently encountered major diseases of the human body.
Of the dyspeptic pains, that of gastritis, duodenitis, and heartburn should be treated with an increase in water intake alone. When there is associated ulceration, attention to the daily diet to enhance the rate of repair of the ulcer site becomes necessary.
According to Professor Howard Spiro of
It is the pain associated with these differently classified conditions that forces the person to consult a medical practitioner. It is this pain that is now getting much attention even though many different jargons are attached to the local conditions seen through the endoscope. The common factor is the dyspeptic pain. The local tissue change is the descriptive explanation for the changes brought about by the basic common factor, namely the initiating dehydration.
How am I able to make such claims? I have treated with only water well over 3000 persons with dyspeptic pain who had other distinguishing characteristics to classify them according to those jargons. They all responded to an increase in their water intake, and their clinical problems associated with the pain disappeared. The report of my new way of treating dyspeptic pain with water was published as the editorial article in the Journal of Clinical Gastroenterology in June of 1983.
At a certain threshold of dehydration, when the body urgently calls for water, nothing else can substitute. No medication other than water is effective. One of the many patients I treated with water stands out and proves this fact. He was a young man in his middle twenties. He had suffered from peptic ulcer disease for a number of years before the crisis time, when I met him. He had the usual diagnostic procedures performed on him and received the label of 'duodenal ulcer.' He had been given antacids and brand name cimetidine medications.
Cimetidine is a form of very strong medication that blocks the action of histamine on its '2nd' type receiver points, generally known as 'receptors' in the body, and, in this case, known as histamine 2 or Hz receptor. It just happens that some cells in the stomach that produce the acid are sensitive to this medication. However, many, many other cells in the body that do not produce acid are also sensitive to this blocking action of the medication. That is why this medication has many other side effects, (including impotence in the young) and has proven extremely dangerous in the chronically dehydrated older age group.
The first time I set eyes on the young man was at eleven one evening in the summer of 1980. He was in such pain that he was almost semiconscious. He was lying folded in the fetal position on the floor of his room. He was groaning steadily, unaware of his environment and the worried people around him. When I talked to him, he did not respond. He was not communicating with those around him. I had to shake him to get a response.
I asked him what was the matter. He groaned, 'My ulcer is killing me.' I asked him how long he had had the pain. He said his pain started at one in the afternoon, immediately after his lunch. The pain increased in intensity as time passed. I asked him what he had done to get relief and if he had taken any medication. He replied that he had taken three tablets of cimetidine and one whole bottle of antacid during this time. He indicated that he got absolutely no relief, even with this amount of medication, in the ten hours since his pain first started.
When so much medication cannot relieve the pain of peptic ulcer disease, one automatically becomes suspicious of 'acute abdomen,' something that might possibly need surgical exploration. Maybe his ulcer had perforated! I had seen and assisted in the operation of patients with perforated peptic ulcers. Those persons were devastatedvery much like the young man before me. The test is very simple; such patients develop a very rigid abdominal wall, almost like a wooden board. I felt for the rigidity of the wall of the abdomen in this young man. Fortunately, he had not perforated. His abdominal wall was soft, but tender from the pain. He was lucky he had not perforated, although if he had continued like this, the acid would have punched a hole through his now inflamed ulcer.
The arsenal of medications in such circumstances is very limited. Three cimetidine tablets of 300 milligrams each and one full bottle of antacid could not relieve the pain. Often, such cases would end on the operating table of a knife-happy surgeon. Because of my extensive experience with the pain-relieving property of water in dyspeptic pains, I gave this man two full glasses of waterone pint. At first he was reluctant to drink the water. I told him he had taken the usual medications without any result. He should now try 'my medication' for this disease. He had no choice. He was in severe pain and did not know what to do about it. I sat in a corner and observed him for a few minutes.
I had to leave the room, and when I returned in about fifteen minutes, his pain had become less severe and his groans stopped. I gave him another full ,glass of waterhalf a pint. In a few minutes, his pain disappeared completely and he started taking notice of the people around him. He sat up and began to move toward the wall of the room. With his back to the wall, he started to conduct conversations with his visitors who were now more surprised than he at the sudden transformation that three glasses of water had brought about! For 10 hours, this man had suffered from pain and taken the most potent and advanced medicines for the treatment of peptic ulcer disease without any relief. Now, three glasses of water had produced an obvious and absolute relief in about 20 minutes.
If you refer to Figure 4 on page 23 and compare the statements in the model on pain with the experience of the above patient, you will recognize the brain component to the intensity of signaling thirst in the body. After a certain threshold, local painkillers will not be effective. The antacid and hi blocking agent cimetidine did not produce even a reduction in the pain felt by the young man. It was water alone that registered the right message with the brain to abort its call for water, since there was now an unmistakable signal of its adequate presence in the body. The same mode of pain registration is operative in other regions that signal dehydration in any particular individual. People with rheumatoid joint pain should be aware of this particular phenomenon of pain registration at the brain when there is severe dehydration.
I had another occasion to test whether the abdominal pain registration for dehydration was time-dependent or water-volume-dependent. This time, a man was carried by two other persons into the clinic where I was working at the time. The patient could not walk; he was lifted from under his arms by two other persons. He, too, was a peptic ulcer patient in extremely severe upper abdominal or dyspeptic pain. After examination to see that he had not perforated, I gave the patient one full glass of water every hour. He did not achieve total relief in 20 minutes, or even one hour and 20 minutes. He recovered after he had taken three glasses of water. On the average, it takes less severe cases about eight minutes to achieve total pain relief.
It has been shown experimentally that, when we drink one glass of water, it immediately passes into the intestine and is absorbed. However, within one half-hour, almost the same amount of water is secreted into the stomach through its glandular layer in the mucosa. It swells from underneath and gets into the stomach, ready to be used for food breakdown. The act of digestion of solid foods depends on the presence of copious amounts of water. The acid is poured on the food, enzymes are activated, and the food is broken down into a homogenized fluid state that can pass into the intestine for the next phase of digestion.
The mucus covers the glands' layer of the mucosa, which is the innermost layer of the structure of the stomach (see Figure 5). Mucus consists of 98 percent water and two percent the physical 'scaffolding' that traps water. In this 'water layer' called mucus, a natural buffer state is established. The cells below secrete sodium bicarbonate that is trapped in the water layer. As the acid from the stomach tries to go through this protective layer, the bicarbonate neutralizes it.
The outcome of this action is a greater production of salt (sodium from the bicarbonate and chlorine from the acid). Too much salt alters the water-holding properties of the 'scaffolding' material of mucus. Too much acid neutralization and salt deposits in this mucus layer would make it less homogeneous and sticky and would allow the acid to get to the mucosal layer, causing pain.
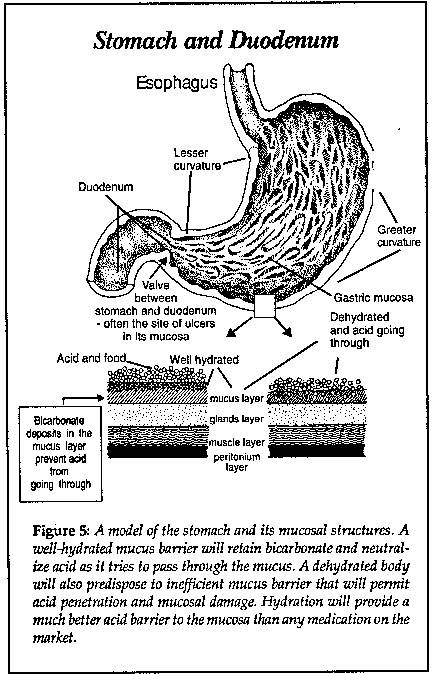
The natural design in the resection of water through the mucus layer seems to be the process of 'back-washing' the mucus layer and getting rid of the salt deposits. This is a most efficient design for rehydrating the mucus layer from the bottom when new mucus is also secreted. This refreshed, thickened and sticky mucus barrier is the natural protective shield against the acid in the stomach. Naturally, the efficiency of this shield depends on a regular intake of water, particularly before the intake of different solid foods that would stimulate the production of acid from the glands in the stomach wall. Thus, water provides the only natural protection against the acid in the stomach, from base upward. Antacids are designed to attach to the acid in the stomach itself an inefficient protection.
We should begin to realize that in the same way we have a 'hunger pain' signal, we also have a 'thirst pain' signal in the body. It is unfortunate they call it 'dyspepsia' and treat it with all sorts of medications until there is local duodenal or stomach tissue damage from the metabolic complications of dehydration. The use of antacids for the relief of this pain is generally the accepted form of treatment. These substances are non-prescription slow poisons that one can buy even in the supermarkets.
Significant research conducted in
Water is most probably the only effective substance to give relief. After all water, and only water, is what the body wants, needs, and is calling for. If we search accurately for other signs, there would be more indicators of dehydration. Do not imagine that dyspeptic pain is the indicator of an isolated and localized phenomenon. In any case, dyspeptic pain is a signal of dehydrationa thirst signalof the body, even if there is an associated ulcer. If water is taken and it relieves your pain, with adequate food intake/ the ulcer is bound to repair itself in due time.
It is now said that ulcers are the result of infections. My researched opinion is that the variety of curved bacteria, blamed for causing ulcerations, are commensals, bacteria that naturally dwell in the intestines. They may take an unfair advantage from the immune system suppression that is the direct outcome of dehydration. You see, the normal intestinal bacteria cohabitate with us and produce much of the vitamins needed by the body. They contribute to our well-being when we are strong. In dehydration, particularly at the site of the valve between the stomach and the duodenum many histamine producing nerves exist. This particular curved bacterium benefits from the growth hormone effects of histamine. at the same time that these nerves are restrictively monitoring the rate of flow of the strongly acidic content of the stomach into the intestine. In any case, not all ulcer sites show the presence of 'helicobacters.' Also, an infinite number of people may have helicobacter in their intestines and not suffer from ulcers!
Antacids that contain aluminum are dangerous. They should not be freely used for a condition that will respond to an increase in water intake. Excessive aluminum in circulation has been very strongly implicated as a precipitating factor on top of other considerations in Alzheimer-type disease. It is imperative to understand this relationship between taking aluminum-containing antacids for a long period of time and its possible accumulative toxic side effect of brain damage in Alzheimer's disease. No amount of genetic study will undo the toxic side effect of a metal used in medications to deal with a simple signal of thirst under a wrong paradigm. Most antacids contain between 150-600 milligrams of aluminum in every spoonful of the liquid, or in each tablet that is chewed.
The
Histamine blocking agents are also not suitable for long-term use. They have many side effects. These include dizziness and confusion states in the elderly. Enlarged breasts appear in men after a few weeks of taking this medication. Low sperm count in some male patients and loss of libido have also been noted. Nursing mothers or pregnant women should not use this type of medication to treat the thirst signals of the bodythe child's and the mother's. Brain capillaries respond to dehydration by dilating if histamine stimulates them. These antihistamines will block the capillary dilating action of histamine when the brain has to tabulate more information than normal, such as when under the pressure of stress. The brain will get less blood supply when antihistamines are used for dyspeptic pain treatment.
The primary cause of Alzheimer's disease is chronic dehydration of the body. In my opinion, brain cell dehydration is the primary cause of Alzheimer disease. Aluminum toxicity is a secondary complication of dehydration in areas of the world with comparatively aluminum-free water. Caution: In the technically advanced Western societies aluminum sulphate is at times used in the process of water purification for delivery into the city water supplies. In prolonged dehydration, the brain cells begin to shrink. Imagine a plum gradually turning into a prune. Unfortunately, in a dehydrated state, many, many functions of brain cells begin to get lost, such as the transport system that delivers neurotransmitters to nerve endings. One of my medical friends took this information to heart and started treating his brother who has Alzheimer's disease by forcing him to take more water every day. His brother has begun to recover his memory, so much so that he can now follow conversation and not frequently repeat himself. The improvement became noticeable in a matter of weeks.
It should be recognized that although pain is localized to the region of the stomach, the dehydration is established all over the body. Not recognizing dyspeptic pain to be a thirst signal calling for water will, later in Me, cause the human body many irreversible problems. Of course, a stomach tumor could cause a similar pain. However, that pain will not disappear with water. It will continue to recur. In case there are repeated pains even when water intake has been regulated for a number of days, it would be prudent to consult a physician for assessment of the condition. If the pain is from gastritis and duodenitis, or even peptic ulcerations, regular intake of water is a must in the daily routine and dietary adjustments for the treatment of the conditions.
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 864
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2024 . All rights reserved