| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Warren et al. (1979) described in his classical article in detail the anatomical structures of the medial side of the knee in three layers.
-Layer (I) is superficial fascia encountered after skin incision, it is part of the deep crural fascia: a thin sheet under the subcutis. It blends with pes anserinus and tibial periosteum distally, it covers the sartorius and quadriceps proximally superior and retinaculum anterior, forms the deep crural fascia posteriorly.
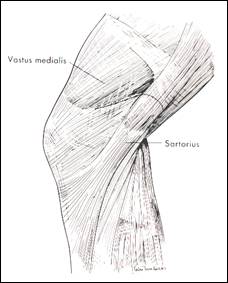
fig 1: layer I superficial crural fascia
-Layer II is the superficial medial collateral ligament (SMCL) with parallel fibers running from the femoral epicondyle to the anteromedial tibial crest 5-7 cm below the joint line. These fibers blends posteriorly with the oblique fibers of layer III, the pes tendons are situated between layer I and II-III. Anterior to the femoral insertion it is continuous with the medial patellofemoral ligament (fig 2a-c).
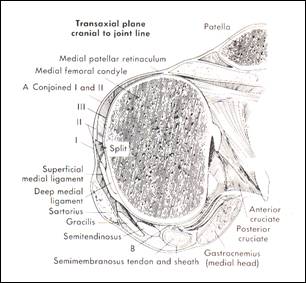
fig 2a 3 layers of the medial capsule and ligaments of the knee at femur
level (from
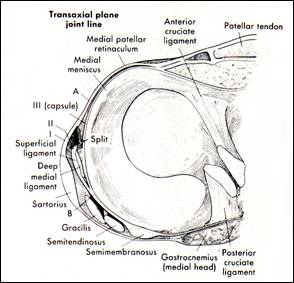
fig 2b The 3 layers of the medial
capsule and ligaments of the knee at joint level (from
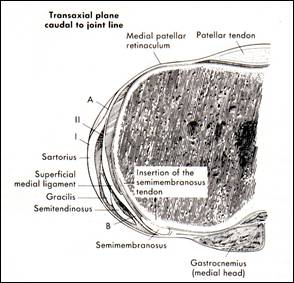
fig 2b The 3 layers of the medial
capsule and ligaments of the knee at tibia level (from
-Layer III is the true capsular layer. It is thin and loose anterior to the SMCL and blends with layer I into the retinaculum. Beneath the SMCL layer III thickens and forms the deep MCL (DMCL) from femur condyle to meniscus and from meniscus to tibia. It allows limited movement of the meniscus. The proximal insertion merges into the SMCL fibers, but sometimes it has a distinct attachment 0.5 cm below. The meniscotibial insertion of the DMCL is clearly separated from the SMCL but blends with it posteriorly (fig 3,4).
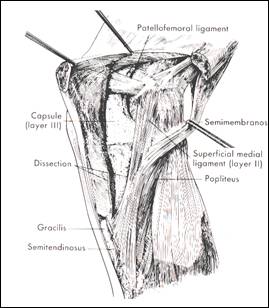
fig 3 Layer I reflected revealing layer II and III (from
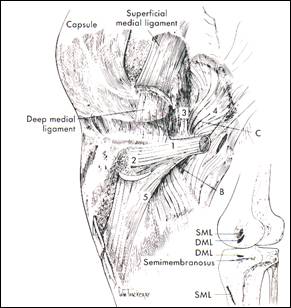
fig. 4 Layer II (SMCL) removed revealing layer III and bony insertions.
1.direct arm, 2.amterior extension, 3.capsular extention, 4.posterior extension,
5.inferior extension semimembranosus tendon sheath (from
The conjoined tissue of Layer II and III form the posteromedial corner (PMC).
This corner is augmented by the semimembranosus tendon which insert in the posteromedial tibia just below the joint line (fig 4).
It has:
- an anterior extension (underneath the MCL)
- a capsular extension of the tendon sheath to the PMC.
- a posterior extension of the tendon sheath to the posterior capsule of the lateral condyle
(forms the oblique popliteal ligament)
-a distal medial tibial extension (to the inferior fibers of the SMCL)
-a distal posterior to the popliteal muscle fascia (Mueller)
Literature
Warren LF, et al. (1979) The Supporting Structures and Layers on the Medial Side of the Knee An Anatomical Analysis. The Journal of Bone and Joint Surgery 61-A (1): 56-62
Mller W, et al. (1983) Form, Function, and Ligament Reconstruction. The Knee (Springer-Verlag)
Hughston JC , et al. (1973) The Role of the Posterior Oblique Ligament in Repairs of Acute Medical (Collateral) Ligament Tears of the Knee. The Journal of Bone and Joint Surgery 55-A (5): 923-940
Ambacher (2000) described with microangiography that one or two vascular bundles provide bloodsupply from the proximal insertion area to distal areas. The vascularisation is more abundant in the proximal femoral area and limited in the distal area below the meniscal insertion. The main artery was frequently in the ventral part of the mcl (52%) but also in the middle (33%) or dorsal part (15%).
Literature
Ambacher T, et al. (2000) Mikroangiographische Darstellung der Gefssversorgung des medialen Kollateralbandes am Kniegelenk. Der Unfallchirurg 103: 208-214
FUNCTIONAL ANALYSIS MEDIAL STRUCTURES OF THE KNEE, BIOMECHANICAL STUDIES.
Mller described in his masterwork The Knee (1983) form and function of the medial ligaments and the posteromedial corner.
The knee can be described as a four-bar linkage system in which the knee is rotating and gliding as guided by the cruciate ligaments situated in the central pivot of the knee. The proximal femoral fibers of the MCL are situated above the central rotating point of the four-bar system and are connected with distal insertion points on the tibia in such a way that the distance remains practically the same. They are situated within the so-called Burmester Curve (fig 5). Fibers within this loop are not overstretched with normal knee movement, fibers outside would be overstretched.
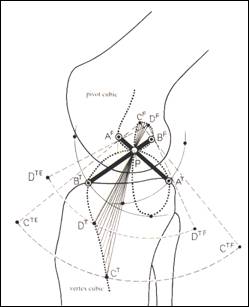
fig.5 Burmester Curve and four-bar linkage system (from Mller 1983)
Mller stated that the most anterior fibers of the SMCL are tensioned in flexion since the insertion site is rotated upwards, the posterior fibers are relaxed and rotate underneath the anterior fibers. Warren et al. (1974) also had found this. Poliacu Prose et al. (1988) found on the femur in extension that anterior fibers of the SMCL are inserted somewhat above and anterior of the epicondyle and the posterior fibers somewhat distally. They found that in flexion the insertion site rotates and anterior and posterior fibers twist around each other while remaining taut in all positions. (fig 6). The DMCL is also tensioned in flexion through rotation of the insertion site on the femur (Mueller 1983, Poliacu Prose 1988).
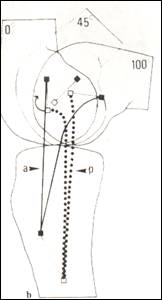
fig.6 mcl fibers twist around insertion
(from Poliacu Prose 1988)
Gardiner (2001) confirmed the above mentioned hypothesis in lab tests. He found with straingauges in the MCL complex that near extension the posterior proximal part of the MCL was tensioned, in 60 degrees of flexion both the anterior and posterior fibers and in 90 degrees of flexion the anterior fibres.
In cutting studies the SMCL is the primary restraint against valgus and transection causes 2-5 degrees laxity in flexion or approximately 3-5 mm joint opening. The total amount of valgus laxity is limited. Additional cutting of the POL/PMC gives additional laxity of 7-8 degrees up to 10 degrees (Grood 1981, Haimes 1994, Nielsen 1984, Nielsen 1984b, Markolf 1976, Warren 1974). The general consensus is that an isolated SMCL lesion causes laxity in flexion, and combination with POL/PMC lesion does also give laxity in extension. An ACL rupture should be suspected when there is a large valgus opening in extension of more than 8 degrees (Haimes 1994).
Hughston (1973) and Mller (1983) described that the tissue of the posteromedial corner is dynamised by the semimembranosus via the various extensions. The fibers of the PMC are outside the Burmester curve and lax in flexion. External rotation is limited by the triangular arrangement of the MCL and the posterior oblique ligament together with menisicus with its tibiofemoral insertion and connection with the semimembransosus tendon (fig 7).The POL acts also as an indirect synergist for the ACL via the meniscal-tibial complex.
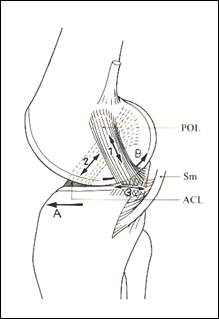
fig 7 the POL meniscus tibia complex limits external rotation (from Mller 1983)
The fibers of the POL are parallel to the PCL (fig 8) and resist posterior translation and internal rotation.
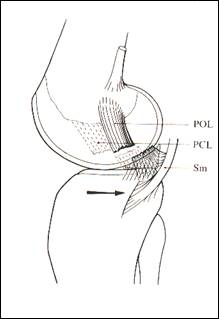
fig 8 the POL is a synergist of the PCL (from Mller 1983)
Cutting studies confirm that the SMCL is also the primary restraint to external rotation (Warren 1974, Nielsen 1984b, Markolf 1976, Haimes 1999, Sullivan 1984, Shoemaker 1985). Cutting the SMCL increases external rotation 4-10 degrees with the largest increase in flexion. The internal rotation does not increase. Additional cutting of the POL/PMC above the SMCL does add 5-10 degrees to the external rotation. Also the internal rotation increases considerably after additionally cutting the posteromedial complex (Haimes 1994, Nielsen 1984b) .
In case of ACL deficiency a lesion of the SMCL also causes increased anterior laxity especially in 90 degrees of flexion (Sullivan 1984, Haimes 1994, Shoemaker 1985). Additional cutting of the POL/PMC adds to this increased anterior laxity . In these ACL deficient knees an extreme large valgus laxity ( >13 degrees) will be found.
Summarizing the effects of lesions of the various medial ligament structures:
-An SMCL rupture causes 2-5 degrees valgus joint opening in flexion of the knee and 4-10 degrees increased external rotation in flexion of the knee. The knee is stable in extension.
-A DMCL rupture on the femoral side occurs usually in combination with SMCL lesion. The DMCL does not play an important role in valgus stability.
-A DMCL lesion at the meniscotibial side increases the mobility of the medial meniscus.
-A rupture of the POL/PMC occurs in combination with SMCL lesions. It causes 7-8 degrees more laxity in flexion in addition to the laxity caused by the SMCL lesion. The laxity is also present in extension. The external rotation increases 10-20 degrees in flexion and the internal rotation in also increased. The meniscotibial fibers in the posteromedial corner can be ruptured and will cause increased mobility of the meniscus.
-In case of an ACL deficiency MCL/PMC lesions cause an increase of the anterior laxity especially in 90 degrees of flexion. Also an extreme large valgus laxity is found.
Literature:
Mller W, et al. (1983) Form, Function, and Ligament Reconstruction. The Knee (Springer-Verlag)
Warren LF, et al. (1974) The Prime Static Stabilizer of the Medial Side of the Knee. The Journal of Bone and Joint Surgery 56-A (4): 665-674
Poliacu Pros L, et al. (1988) The Collateral Ligament of the Knee Joint in the Cat and Man Morphological and Functional Study of the Internal Arrangement of Fibers. Acta Anat. 133: 70-78
Gardiner JC, et al. (2001) Strain in the Human Medial Collateral Ligament During Valgus Loading of the Knee. Clinical Orthopaedics and Related Research 391: 266-274
Grood ES, et al. (1981) Ligamentous and Capsular Restraints Preventing Straight Medial and Lateral Laxity in Intact Human Cadaver Knees. The Journal of Bone and Joint Sugery 63-A: 1257-1269
Haimes JL, et al. (1994) Role of the Medial Structures in the Intact and Anterior Cruciate Ligament-Deficient Knee Limits of Motion in the Human Kne. The American Journal of Sports Medicine 22 (3): 402-409
Nielsen S, et al. (1984) Instability of Cadever Knees after Transection of Capsule and Ligaments. Acta Orthop. Scand.
Nielsen S, et al. (1984) Rotatory Instability of Cadaver Knees after Transection of Collateral Ligaments and Capsule. Arch. Orthop.Trauma Surg. 103: 165-169
Markolf KL, et al. (1976) Stiffness and Laxity of the Knee The Contributions of the Supporting Structures A Quantitative in Vitro Study. The Journal of Bone and Joint Surgery 58-A (5): 583-593
Hughston JC , et al. (1973) The Role of the Posterior Oblique Ligament in Repairs of Acute Medical (Collateral) Ligament Tears of the Knee. The Journal of Bone and Joint Surgery 55-A (5): 923-940
Shoemaker SC, et al. (1985) Effects of Joint Load on the Stiffness and Laxity of Ligament-Deficient Knees An in Vitro Study of the Anterior Cruciate and Medial Collateral Ligaments. The Journal of Bone and Joint Surgery 67-A (1): 136-146
Sullivan D, et al. (1984) Medial Restraints to Anterior-Posterior Motion of the Knee. The Journal of Bone and Joint Surgery 66-A (6): 930-936
DIAGNOSIS
Clicical testing with valgus laxity in flexion indicates a lesion of the SMCL. Valgus laxity in extension indicates a lesion of both the SMCL and POL/PMC. With large opening the cruciates could also be damaged.
Many authors use the following grading of the MCL lesion: Grade I ( first degree sprain with minimal disruption of fibers, tenderness, solid end point ) 0-5 mm laxity . Grade II (2nd degree sprain with more fiber disruption, firm endpoint) 5-10 mm laxity in flexion. Grade III (complete rupture, no endpoint) > 10 mm opening of the joint in flexion and extension. (Ritchie 1994, Shelbourne 1995, Scuderi 1993).
From this somewhat imprecise grading of MCL lesions it is not clear which ligament is ruptured. Noyes (1995) Hillard-Sembel (1996), Spindler (1994) and Fetto (1978) proposed abduction testing in 0 and 20 degrees of flexion. Their modified (and more precise) grading of MCL lesions based on the cutting studies ( Grood 1981, Haimes 1994, Warren 1974) and measures left-right differences.
-Grade I lesion: tenderness , solid endpoint , no increase in laxity
-Grade II lesion: an increased 3-5mm valgus laxity measured in 20 degrees of flexion with a firm endpoint, this represents an SMCL rupture. The knee is stable in extension.
-Grade III lesion: causes more than 5 mm additional joint opening in 20 degrees of flexion without an end point. It represent and MCL and also POL/PMC rupture. There is laxity in extension. According to Hughston (1973) this grade III laxity can be 1+ (<5mm), 2+ (6-10 mm) and 3+ (>10 mm)
MRI analysis can visualize the medial capsular structures adequately (Maeseneer 2000, Loredo 1999). MR grading of acute medial capsular lesions however may not be completely accurate for clinical classification of the MCL and PMC lesions (Schweitzer 1995) although Rasenberg et al. ( 1995) did find a correlation between MRI grade III lesions (rupture) and increased instrumented laxity measurements.
Stress radiograms can document valgus laxity (Jacobsen 1976, Balmer 1988, Kennedy 1971, Hillard-Sembel 1996) and Ultrasound can also be used for laxity measurement (Gruber 1998).
Literature:
Ritchie JR, et al. (1994) History and Physical Evaluation. Knee Surgery (Ed. Fu, et al..), Williams & Wilkins: 253-273
Shelbourne KD, et al. (1995) Management of Combined Injuries of the Anterior Cruciate and Medial Collateral Ligaments . The Journal of Bone and Joint Surgery 77-A (5): 800-806
Scuderi GR, et al. (1993) Classification of Knee Ligament Injuries. Surgery of the Knee second edition (Ed. Insall, et al..), Churchill Livingstone: 387-401
De Maeseneer M, et al. (2000) Three Layers of the Medial Capsular and Supporting Structures of the Knee: MR Imaging-Anatomic Correlation. RadioGraphics 20:S83-S89
Loredo R, et al. (1999) Posteromedial Corner of the Knee: MR Imaging with Gross Anatomic Correlation. Skeletal Radiol. 28: 305-311
Schweitzer ME, et al. (1995) Medial Collateral Ligament Injuries: Evaluation of Multiple Signs, Prevalence and Location of Associated Bone Bruises, and Assessment with MR Imaging. Radiology 194: 825-829
Rasenberg EIJ, et al. (1995) Grading Medial Collateral Ligament Injury: Comparison of MR Imaging and Instrumented Valgus-varus Laxity Test-device. A Prospective Double-blind Patient Study. European Journal of Radiology 21: 18-24
Jacobsen K (1976) Stress Radiographical Measurement of the Anteroposterior, Medial and Lateral Stability of the Knee Joint. Acta orthop. scand.
Gruber G, et al. (1998) Stellenwert der sonographischen Untersuchung bei Lsion des medialen Knie-Seitenbandapparates. Z. Orthop. 136: 337-342
Ballmer PM, et al.. (1988) The Non Operative Treatment of Isolated Complete Tears of the Medial Collateral Ligament of the Knee. Arch. Orthop. Trauma Surg. 107: 273-276
Kennedy JC, et al.. (1971) Medial and Anterior Instability of the Knee. An Anatomical and Clinical Study using Stress Machines. The Journal of Bone and Joint Surgery 53-A: 1257-1270
Hillard-Sembel D, et al.. (1996) Combined Injuries of the Anterior Cruciate and Medial Collateral Ligaments of the Knee. The Journal of Bone and Joint Surgery 78-A (2): 169-176
Noyes FR, et al.. (1995) The Treatment of Acute Combined Ruptures of the Anterior Cruciate and Medial Ligaments of the Knee. The American Journal of Sports Medicine 23 (4): 380-391
Spindler KP, et al.. (1994) General Approach to Ligament Surgery (Ed. Fu, et al..) Williams & Wilkens: 655-665
Fetto JF, et al. (1978) Medial Collateral Ligament Injuries of the Knee: A Rationale for Treatment. Clinical Orthopaedics and Related Research 132: 207-218
Grood ES, et al. (1981) Ligamentous and Capsular Restraints Preventing Straight Medial and Lateral Laxity in Intact Human Cadaver Knees. The Journal of Bone and Joint Sugery 63-A: 1257-1269
Warren LF, et al. (1974) The Prime Static Stabilizer of the Medial Side of the Knee. The Journal of Bone and Joint Surgery 56-A (4): 665-674
Haimes JL, et al. (1994) Role of the Medial Structures in the Intact and Anterior Cruciate Ligament-Deficient Knee Limits of Motion in the Human Kne. The American Journal of Sports Medicine 22 (3): 402-409
RESULTS OF CONSERVATIVE AND OPERATIVE TREATMENT AND INDICATIONS FOR OPERATIVE TREATMENT IN ACUTE INJURIES.
Isolated grade II lesions will heal with conservative treatment although a small percentage of patient have some residual laxity. Most patients have good knee funtion and sporting ability. (Fetto 1997, Derscheid 1981, Holden 1983, Lundberg 1994, Indelicato 1983, 1989, Kannus 1988, Petermann 1993)
With longer follow-up limited degerative radiographic changes are seen but no joint narrowing (Kannus 1988, Lundberg 1996) .
Isolated grade III lesions will also heal with functional conservative treatment (Indelicato 1995, Reider 1993, Indelicato 1983, 1990, Jones 1986, Balmer 1988, Peterman 1993). Fetto (1978) and Sandberg (1987) found no improvement after operative treatment of isolated grade III lesions. Some patients have residual laxity usually in flexion. Kannus (1988) found at longer follow-up after conservative treatment a much higher percentage of instability and osteoarthrosis in grade III MCL lesions but his data show that probably many patients had also ACL lesions. Kannus thought surgical treatment might improve results. Hughston (1973 ) also strongly advocates repair of the medial structures and reports good results.
Combined MCL- ACL lesions have a worse prognosis with respect to residual laxity and osteoarthritis. The role of surgery remains controversial.
Mok (1989) et al. treated grade III MCL /ACL lesions conservative with excellent short term results.
Fetto (1979) found better results with operative treatment of all the ligament lesions compared to conservative treatment.
Sandberg (1987) also found worse result in combined lesions but could not prove the benefit of repair in his randomised trail, he repaired in a subgroup all ligament lesions.
Robins (1993) found more limited knee function in patients who had an ACL reconstruction and repair of the proximal MCL lesion. Better return to motion was found in patients with a distal MCL lesion.
Shirakura (2000) found better functional results if in combined lesions the MCL was repaired versus conservative treatment. Nakamura. ( found residual valgus laxity in patients who had an acl repair and a conservatively treated MRI grade III MCL lesion.
Hughston (1973, 1994) advocated operative treatment and claims good results with MCL/POL repair without ACL in combined lesions, he had no control group.
Hillard-Sembel (1996) found comparable results for MCL healing after repairing both MCL/ACL or only ACL reconstruction or without operative treatment.
Noyes (1995) found after ACL reconstruction and repair of grade III MCL lesions worse results and more complications and stiffness than after ACL repair and leaving a grade II MCL lesion alone.
In conclusion isolated grade II and III can be treated conservatively. In acute combined MCL/ACL lesions first a functional treatment of the MCL lesion is now proposed and if needed subsequent later repair ACL reconstruction after 8-10 weeks after regaining knee function is advocated. This will prevent knee stiffness and improve patient satisfaction (Noyes 1995, Petersen Shelbourne 92). Also for the Posterior Cruciate lesions in combination to MCL lesions this approach is advocated by Shelbourne (2003). Contrary to the ACL the PCL has some potential to heal.
Indications for operative treatment in acute phase are limited to global instability, bony ligament avulsions, dislocation of a ligament in the joint and dislocation of the meniscus (Lobenhoffer 2002).
Chronic instability of the MCL/PMC is a relative rare operation indication (Baker 94). Many non -anatomic procedures have been described but these failed at longer follow-up.
(Linton 1994, oDonoghue 1973, Nicholas 1973).
Recent literature on operative treatment of chronic MCL/PMC lesions is scarce. Hughston (1973) and Mueller (1983) described anatomic repair of the MCL/PMC with retensioning and reattachement of the ligaments and refixation of the semimembranosus tendon and preservation of the meniscus. Shahane et al. (98) reported favourable results after an isometric proximal advancement and recession of the MCL. Kim et al. (2001) and Borden (2002) reported anatomic-like reconstructions with semitendinosus tenodesis for repair of the SMCL and POL but results were not available. A strip of semitendinosus tendon can also be used to support the POL (Mueller 1983).
Cameron et al. (94) stressed the importance of valgus alignment in symptomatic medial instability . He proposed various osteotomy techniques for correction of the axis and retensioning of the ligament.
Literature:
Fetto JF, et al. (1978) Medial Collateral Ligament Injuries of the Knee: A Rationale for Treatment. Clinical Orthopaedics and Related Research 132: 207-218
Derscheid GL, et al. (1981) Medial Collateral Ligament Injuries in Football Nonoperative Management of Grade I and Grade II Sprains. The American Journal of Sports Medicine 9(6): 365-368
Holden DL, et al. (1983) The Nonoperative Treatment of Grade I and II Medial Collateral Ligament Injuries To The Knee. The American Journal of Sports Medicine 11(5): 340-343
Lundberg
M, et al. (1994) Decrease in Valgus Stiffness After
Medial Knee Ligament Injury A 4-Year Clinical and Mechanical Follow-Up Study
in 38 Patients. Acta Orthopaedica
Indelicato PA, et al. (1983) Non-Operative Treatment of Complete Tears of the Medial Collateral Ligament of the Knee. The Journal of Bone and Joint Surgery 65-A(3): 323-329
Indelicato PA, et al. (1989) Nonoperative Management of Complete Tears of the Medial Collateral Ligament of the Knee in Intercollegiate Football Players. Clinical Orthopaedics and Related Research 256: 174-177
Kannus P, et al. (1988) Osteoarthrosis in a Knee Joint Due to Chronic Posttraumatic Insufficiency of the Medial Collateral Ligament. Nine-Years Follow-Up. Clinical Rheumatology 2: 200-207
Petermann J, et al. (1993) Non-Operative Treatment of Acute Medial Collateral Ligament Lesions of the Knee Joint. Knee Surgery Sports Traumatology Arthroscopy 1: 93-96
Kannus P (1988) Long-Term Results of Conservatively Treated Medial Collateral Ligament Injuries of the Knee Joint. clinical Orthopaedics and Related Research 226: 103-112
Lundberg M, et al. (1996) Long-Term Prognosis of Isolated Partial Medial Collateral Ligament Ruptures A Ten-Year Clinical and Radiographic Evaluation of a Prospectively Observed Group of Patients. The American Journal of Sports Medicine 24(2): 160-163
Indelicato PA (1995) Isolated Medial Collateral
Ligament Injuries in the Knee. Journal of
Sandberg R, et al. (1987) Operative Versus Non-Operative Treatment of Recent Injuries to the Ligament of the Knee. The Journal of Bone and Joint Surgery 69-A(8): 1120-1126
Reider B, et al. (1993) Treatment of Isolated Medial Collateral Ligament Injuries in Athletes With Early Functional Rehabilitation A Five-year Follow-up Study. the American Journal of Sports Medicine 22(4): 470-477
Jones RE, et al. (1986) Nonoperative Management of Isolated Grade III Collateral Ligament Injury in High School Football Players. Clinical Orthopaedics and Related Research 213: 137-140
Ballmer PM, et al. (1988) The Non Operative Treatment of Isolated Complete Tears of the Medial Collateral Ligament of the Knee A Prospective Study. Archives of Orthopaedic and Traumatic Surgery 107: 273-276
Hughston JC, et al. (1973) The Role of the Posterior Oblique Ligament in Repairs of Acute Medial (Collateral) Ligament Tears of the Knee. The Journal of bone and Joint Surgery 55-A(5): 923-940
Hughston JC, et al. (1994) The Importance of the Posterior Oblique Ligament in Repairs of Acute Tears of the Medial Ligaments in Knees with and without an Associated Rupture of the Anterior Cruciate Ligament Results of Long-Term follow-Up. The Journal of Bone and Joint Surgery 76-A(9): 1328-1344
Mok DWH, Good C, (1989) Non-operative management of acute grade III medial collateral ligament injury of the knee: a prospective study. Injury 20, 277-280.
Robins AJ, et al. (1993) Postoperative Return of Motion in Anterior Cruciate Ligament and Medial Collateral Ligament Injuries The Effect of Medial Collateral Ligament rupture Location. The American Journal of Sports Medicine 21(1): 20-25
Shirakura K (2000) The Management of Medial Ligament Tears in Patients with Combined Anterior Cruciate and Medial Ligament Lesions. International Orthopaedics (SICOT) 24: 108-111
Nakamura N, et al. (2003) Acute Grade III Medial Collateral Ligament Injury of the Knee Associated with Anterior Cruciate Ligament Tear The Usefulness of Magnetic Resonance Imaging in Determining a Treatment Regimen. American Journal of Sports Medicine 31(2): 261-267
Hillard-Sembell D, et al. (1996) Combined Injuries of the Anterior Cruciate and Medial Collateral Ligaments of the Knee Effect of Treatment on Stability and Function of the Joint. The Journal of Bone and Joint Surgery 78-A(2): 169-176
Noyes FR, et al. (1995) The Treatment of Acute Combined Ruptures of the Anterior Cruciate and Medial Ligaments of the Knee. The American Journal of Sports Medicine 23(4): 380-391
Petersen W, et al. (1999) Combined Injuries of the Medial Collateral Ligament and the Anterior Cruciate Ligament Early ACL Reconstruction Versus Late ACL Reconstruction. Arch Orthop Trauma Surg 119: 258-262
Shelbourne KD, et al. (1992) Anterior Cruciate Ligament-Medial Collateral Ligament Injury: Nonoperative Management of Medial Collateral Ligament Tears with Anterior Cruciate Ligament Reconstruction A Preliminary Report. The American Journal of Sports Medicine 20(3): 283-286
Shelbourne KD, et al. (2003) Combined Anterior and Posterior Cruciate and Medial Collateral Ligament Injury: Nonsurgical and Delayed Surgical Treatment. AAOS Instructional Course Lectures 52: 413-417
Lobenhoffer P. (2002) Komplexe Vordere Knieinstabilitt. Orthopde 31: 770-777
Baker CL, et al. (1994) Collateral Ligament Injuries of the Knee: Operative and Nonoperative Approaches. Knee Surgery (Ed. Fu, et al.), Williams & Wilkins: 787-808
Linton RD, et al.(1994) Medial Ligament Injuries. Orthopaedic Sports Medicine (DeLee, et al.), W.B. Saunders Company
ODonoghue DH, et al. (1973) Reconstruction for Medial Instability of the Knee Technique and Results in Sixty Cases. The Journal of Bone and Joint Surgery 55-A(5): 941-946
Nicholas JA, et al. (1973) The Five-One Reconstruction for Anteriomedial Instability of the Knee. The Journal of Bone and Joint Surgery 55-A(5): 899-913
Mller W, et al. (1983) Form, Function, and Ligament Reconstruction. The Knee (Springer-Verlag)
Shahane SA, et al. (1998) Proximal advancement of the Medial collateral Ligament for Chronic Medial Instability of the Knee Joint. The Knee 5: 191-197
Kim SJ, et al. (2001) Semitendinosus Tenodesis for Medial Instability of the Knee. The Journal of Arthroscopic and Related Surgery 17(6): 660-663
Borden PS, et al. (2002) Medial Collateral Ligament Reconstruction With Allograft Using a Double-Bundle Technique. The Journal of Arthroscopic and Related Surgery 18(4): 1-6
Cameron JC, et al. (1994) Management of Medial Collateral Ligament
Laxity. Orthopedic Clinicals of
HOW TO REPAIR A LIGAMENT WITH SURGERY
Bony avulsions can be fixed with washer and screw.
Ligamentous avulsions can be fixed at the anatomical insertion site with trans-osseous non-resorbable sutures or bone anchors or screws with toothed washers. Anchoring ligaments beneath a raised flap of bone is also effective. A distalisation of a ligament insertion (SMCL) with its bony attachment is also an elegant solution (Miller 1998)
Bartel (1977) and Wirth (1980) however have shown that proximalisation of the femoral SMCL insertion causes high strains on the ligament fibers during motion which will lead to failure of the reconstruction. Distalisation on the tibia in the direction of the fibers will not cause these effects if the knee is tensioned in 30 degrees of flexion. The insertion site should remain within the Burmester curve (Mueller 1983).
If the surgeon wants to tension the SMCL at the femoral side, the bony insertion with the ligament attached to it can be recessed at its original position as Shahane (1998) et al. proposed. This recession which will not cause a change of isometry of the fibers.
Stretched tissue can be retensioned by imbrication, non resorbable square or mattress sutures are used for strength where tension is the greatest. These sutures must be carefully aligned with the ligament fibers and are tested during joint motion. Absorbable sutures are used in non-tension areas. (Miller 1998, Mller 1983)
Literature:
Miller RH, et al. (1998) Knee Injuries.
Bartel DL, et al. (1977) Surgical Repositioning of the Medial Collateral Ligament. The Journal of Bone and Joint Surgery 59-A (1): 107-116
Wirth CJ, et al. (1980) Biomechanic Studies Reinserting the Medial Collateral Ligament to Correct a Chronic Anteromedial Instability of the Knee Joint. Arch. Orthop. Traumat. Surg. 96: 171-176
Mller W, et al. (1983) Form, Function, and Ligament Reconstruction. The Knee (Springer-Verlag)
The goal of MCL-PMC reconstruction should be functional anatomical repair of the pathology and retention of the meniscus. After treating the pathology the medial side of the knee should be:
-stable in extension (by repair PMC-POL)
-stable in flexion (by repair SMCL, DMCL)
-stable for external rotation (by repair SMCL, DMCL, meniscotibial fixation, PMC-POL)
-stable for internal rotation (by repair PMC-POL)
-should be dynamised by the semimembranosus tendon (by repair extensions tendon to PMC)
Preoperatively the valgus laxity should be documented in 20 degrees of flexion and extension (clinical, stress x-rays). Also external and internal rotation differences should be registered. Other pathology such as cruciate lesions should be looked for
The following operative steps are suggested:
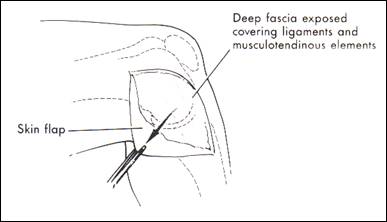
fig. 9 incision layer I fascia (from Miller 1998)
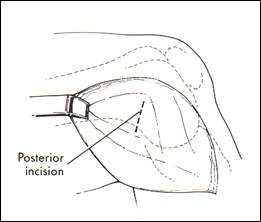
fig. 10 oblique posteromedial incision (from Miller 98)
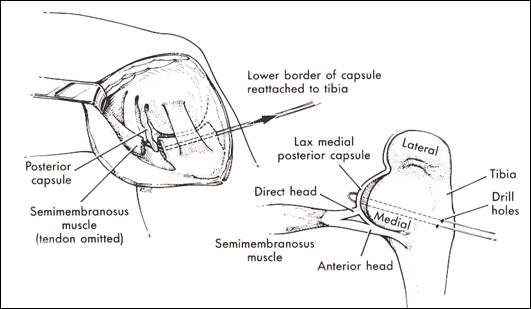
fig. 11 repair semimembranosus and PMC to tibia. Refixation meniscus is not shown (from Miller 1998)
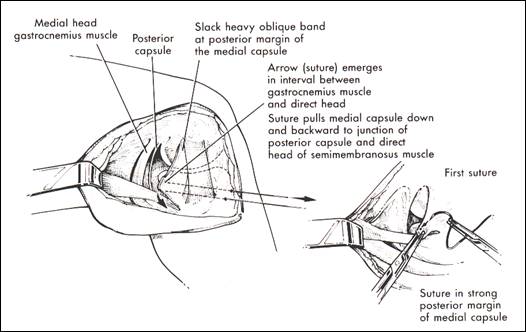
fig. 12 tensioning of the POL (from Miller 98)
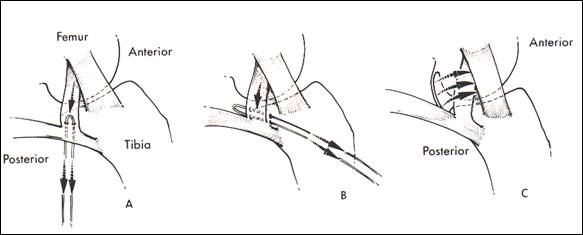
Fig. 13 a.suture through direct arm semimembranosus b.transosseous drillholes c.posterior capsule tensioned over posteromedial capsule (from Miller 98)
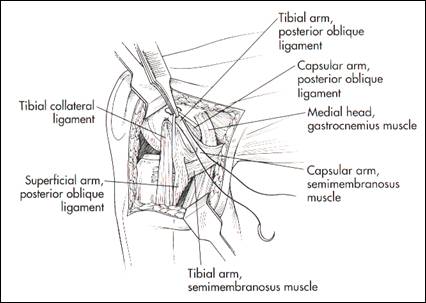
fig. 14 repair POL at femoral insertion (from Hughston 94)
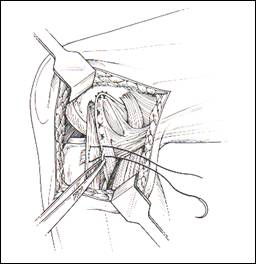
fig. 15 lax capsule is pulled anterior and sutured (from Hughston 94)
Literature:
Miller RH, et al. (1998) Knee Injuries.
Mller W, et al. (1983) Form, Function, and Ligament Reconstruction. The Knee (Springer-Verlag)
Hughston JC, et al. (1994) The Importance of the Posterior Oblique Ligament in Repairs of Acute Tears of the Medial Ligaments in Knees with and without an Associated Rupture of the Anterior Cruciate Ligament Results of Long-Term follow-Up. The Journal of Bone and Joint Surgery 76-A(9): 1328-1344
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 4661
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2024 . All rights reserved