| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Drug Addiction and Drug Abuse
Overview
|
Drugs are so commonly used and abused in modern society that virtually everyone has some familiarity with the concepts of drug addiction and abuse. The term addiction has entered everyday language and often is used to describe behavior that does not involve drug use. For example, the media speak of 'addiction' to sex, running, shopping, or TV. While there certainly can be a superficial resemblance among many varieties of compulsive behavior, there currently is no scientific basis to lump these activities with drug abuse and addiction. These are medical diagnoses with specific criteria that provide the same level of interevaluator reliability as for other medical conditions. Inappropriate use of any drug can be either intentional or inadvertent. Drugs that affect behavior are particularly likely to be taken in excess when the behavioral effects are considered pleasurable. Psychosocial factors tend to be similar for diverse pharmacological agents and are of equal importance in the pathogenesis of these disorders as the unique pharmacological profiles of given drugs. Nevertheless, this chapter focuses on the pharmacological aspects of drug abuse and dependence, including legal prescription drugs, illegal drugs such as heroin or cocaine, and nonprescription drugs such as ethanol and nicotine (see also Chapters 9: Agents Acting at the Neuromuscular Junction and Autonomic Ganglia, 17: Hypnotics and Sedatives, 18: Ethanol, and 23: Opioid Analgesics). |
Drug Dependence
|
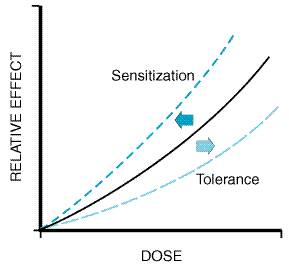
There are many misunderstandings about the origins and even the definitions of drug abuse and addiction. Although many physicians are concerned about 'creating addicts,' very few individuals begin their drug addiction problems by misuse of prescription drugs. Confusion exists because the correct use of prescribed medications for pain, anxiety, and even hypertension commonly produces tolerance and physical dependence. These are normal physiological adaptations to repeated use of drugs from many different categories. Tolerance and physical dependence are explained in more detail later, but it must be emphasized that they do not imply abuse or addiction. This distinction is important, because patients with pain are sometimes deprived of adequate opioid medication simply because they have shown evidence of tolerance and they exhibit withdrawal symptoms if the analgesic medication is abruptly stopped. Definitions Abuse and addiction have been defined and redefined by several organizations over the past 30 years. The reason for these revisions and disagreements is that abuse and addiction are behavioral syndromes that exist along a continuum from minimal use to abuse to addictive use. While tolerance and physical dependence are biological phenomena that can be defined precisely in the laboratory and diagnosed accurately in the clinic, there is an arbitrary aspect to the definitions of the overall behavioral syndromes of abuse and addiction. The most influential system of diagnosis for mental disorders is that published by the American Psychiatric Association (APA) (DSM-IV, 1994). The APA diagnostic system uses the term substance dependence instead of addiction for the overall behavioral syndrome. It also applies the same general criteria to all types of drugs, regardless of their pharmacological class. Although widely accepted, this terminology can lead to confusion between physical dependence and psychological dependence. The term addiction, when used in this chapter, refers to compulsive drug usethe entire substance dependence syndrome as defined in DSM-IV. This should not be confused with physical dependence alone, a common error among physicians. Addiction is not used as a pejorative term but rather for clarity of communication; in fact, the journal Addiction is one of the oldest scientific journals in this therapeutic area. The APA defines substance dependence (addiction) as a cluster of symptoms indicating that the individual continues use of the substance despite significant substance-related problems. Evidence of tolerance and withdrawal symptoms is included in the list of symptoms, but neither tolerance nor withdrawal is necessary or sufficient for a diagnosis of substance dependence. Dependence (addiction) requires three or more of the symptoms, while 'abuse' can be diagnosed when only one or two symptoms are present. Origins of Substance Dependence Many variables operate simultaneously to influence the likelihood of any given person becoming a drug abuser or an addict. These variables can be organized into three categories: agent (drug), host (user), and environment (see Table 241). Agent (Drug) Variables Drugs vary in their ability to produce immediate good feelings in the user. Drugs that reliably produce intensely pleasant feelings (euphoria) are more likely to be taken repeatedly. Reinforcement refers to the ability of drugs to produce effects that make the user wish to take them again. The more strongly reinforcing a drug is, the greater the likelihood that the drug will be abused. Reinforcing properties of a drug can be reliably measured in animals. Generally, animals such as rats or monkeys equipped with intravenous catheters connected to lever-regulated pumps will work to obtain injections of the same drugs in roughly the same order of potency that human beings will. Thus, medications can be screened for their potential for abuse in human beings by the use of animal models. Reinforcing properties of drugs are associated with their ability to increase levels of the neurotransmitters in critical brain areas (see Chapter 12: Neurotransmission and the Central Nervous System). Cocaine, amphetamine, ethanol, opioids, and nicotine all reliably increase extracellular fluid dopamine levels in the nucleus accumbens region. Brain microdialysis permits sampling of extracellular fluid while animals, usually rats, are freely moving or receiving drugs. Smaller increases in dopamine in the nucleus accumbens also are observed when the rat is presented with sweet foods or a sexual partner. In contrast, drugs that block dopamine receptors generally produce bad feelings, i.e., dysphoric effects. Neither animals nor human beings will take such drugs spontaneously. Despite strong correlative findings, a causal relationship between dopamine and euphoria/dysphoria has not been established, and other findings emphasize additional roles of noradrenergic, serotonergic, opioidergic, and GABAergic mechanisms in mediating the reinforcing effects of drugs. The abuse liability of a drug is enhanced by rapidity of onset, since effects that occur soon after administration are more likely to initiate the chain of events that lead to loss of control over drug taking. The pharmacokinetic variables that influence the time it takes the drug to reach critical receptor sites in the brain are explained in more detail in Chapter 1: Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, and Elimination. The history of cocaine use illustrates the changes in abuse liability of the same compound, depending on the form and the route of administration. Coca leaves can be chewed, and the alkaloidal cocaine is slowly absorbed through the buccal mucosa. This method produces low cocaine blood levels and correspondingly low levels in the brain. The mild stimulant effects produced by the chewing of coca leaves have a gradual onset, and this practice has produced little, if any, abuse or dependence despite use over thousands of years by natives of the Andes mountains. Beginning in the late nineteenth century, scientists isolated cocaine hydrochloride from coca leaves, and the extraction of pure cocaine became possible. Cocaine could be taken in higher doses by oral ingestion (gastrointestinal absorption) or by absorption through the nasal mucosa, producing higher cocaine levels in the blood and a more rapid onset of stimulation. Subsequently, it was found that a solution of cocaine hydrochloride could be administered via the intravenous route, giving the ultimate in rapidity of blood levels and speed of onset of stimulatory effects. Each newly available cocaine preparation that provided greater speed of onset and an increment in blood level was paralleled by a greater likelihood to produce addiction. In the 1980s, the availability of cocaine to the American public was increased further with the invention of crack cocaine. Crack, sold at a very low street price ($1 to $3 per dose), is alkaloidal cocaine (free base) that can be readily vaporized by heating. Simply inhaling the vapors produces blood levels comparable to those resulting from intravenous cocaine due to the large surface area for absorption into the pulmonary circulation following inhalation. The cocaine-containing blood then enters the left side of the heart and reaches the cerebral circulation without dilution by the systemic circulation. Inhalation of crack cocaine is thus much more likely to produce addiction than is chewing, drinking, or sniffing cocaine. This method, which rapidly delivers the drug to the brain, also is the preferred route for users of nicotine and cannabis. Although the drug variables are important, they do not fully explain the development of abuse and addiction. Most people who experiment with drugs that have a high risk of producing addiction (addiction liability) do not intensify their drug use and lose control. The risk for developing addiction among those who try nicotine is about twice that for those who try cocaine (Table 242), but this does not imply that the pharmacological addiction liability of nicotine is twice that of cocaine. Rather there are other variables listed in the categories of host factors and environmental conditions that influence the development of addiction. Host (User) Variables In general, effects of drugs vary among individuals. Even blood levels show wide variation when the same dose of a drug on a milligram-per-kilogram basis is given to different people. Polymorphism of the genes that encode enzymes involved in absorption, metabolism, and excretion and in receptor-mediated responses may contribute to the different degrees of reinforcement or euphoria observed among individuals. Children of alcoholics show an increased likelihood of developing alcoholism, even when adopted at birth and raised by nonalcoholic parents (Schuckit, 1999). The studies of genetic influences in this disorder show only an increased risk for developing alcoholism, not a 100% determinism, and this is consistent with a polygenic disorder that has multiple determinants. Even identical twins, who share the same genetic endowment, do not have 100% concordance when one twin is alcoholic. However, the concordance rate for identical twins is much higher than that for fraternal twins. Also of interest is the observation that alcohol and other drug abuse tend to run in the same families, giving rise to postulates that common mechanisms may be involved. Innate tolerance to alcohol may represent a biological trait that contributes to the development of alcoholism. Data from a longitudinal study (Schuckit and Smith, 1996) show that sons of alcoholics have reduced sensitivity to alcohol when compared to other young men of the same age (22 years old) and drinking histories. Sensitivity to alcohol was measured by measuring the effects of two different doses of alcohol in the laboratory on motor performance and subjective feelings of intoxication. When the men were reexamined 10 years later, those who had been most tolerant (insensitive) to alcohol at age 22 were the most likely to be diagnosed as alcohol-dependent at age 32. The presence of tolerance predicted the development of alcoholism even in the group without a family history of alcoholism, but there were far fewer tolerant men in the group with a negative family history. Differences in alcohol metabolism also may influence the propensity for alcohol abuse. Ethanol is metabolized by alcohol dehydrogenase with the production of acetaldehyde, which is then metabolized by a mitochondrial aldehyde dehydrogenase known as ALDH2. A common mutation occurs in the gene for ALDH2, resulting in a less effective aldehyde dehydrogenase. This allele has a high frequency in Asian populations and results in an excess production of acetaldehyde after the ingestion of alcohol. Those who are heterozygous for this allele experience a very unpleasant facial flushing reaction 5 to 10 minutes after ingesting alcohol; the reaction is even more severe in individuals homozygous for the allele, and this genotype has not been found in alcoholics (Higuchi et al., 1996). Similarly, individuals who inherit the gene for impaired nicotine metabolism have been found to have a lower probability of becoming nicotine-dependent. (Pianezza et al., 1998). Psychiatric disorders constitute another category of host variables. Drugs may produce immediate, subjective effects that relieve preexisting symptoms. People with anxiety, depression, insomnia, or even subtle symptoms such as shyness may find, on experimentation or by accident, that certain drugs give them relief. However, the apparent beneficial effects are transient, and repeated use of the drug may lead to tolerance and eventually compulsive, uncontrolled drug use. While psychiatric symptoms commonly are seen in drug abusers presenting for treatment, most of these symptoms started after the person began abusing drugs. Thus, drugs of abuse appear to produce more psychiatric symptoms than they relieve. Environmental Variables Initiating and continuing illicit drug use appear to be significantly influenced by societal norms and peer pressure. Taking drugs may be seen initially as a form of rebellion against authority. In some communities, drug users and drug dealers are role models who seem to be successful and respected; thus, young people emulate them. There also may be a paucity of other options for pleasure or diversion. These factors are particularly important in communities where educational levels are low and job opportunities scarce. Pharmacological Phenomena Tolerance While abuse and addiction are extremely complicated conditions combining the many variables outlined above, there are a number of relevant pharmacological phenomena that occur independently of social and psychological dimensions. First are the changes in the way the body responds to a drug with repeated use. Tolerance is the most common response to repetitive use of the same drug and can be defined as the reduction in response to the drug after repeated administrations. Figure 241 shows an idealized doseresponse curve for an administered drug. As the dose of the drug increases, the observed effect of the drug increases. With repeated use of the drug, however, the curve shifts to the right (tolerance). Thus a higher dose is required to produce the same effect that was once obtained at a lower dose. Diazepam, for example, typically produces sedation at doses of 5 to 10 mg in a first-time user, but those who repeatedly use it to produce a kind of 'high' may become tolerant to doses of several hundreds of milligrams; some abusers have had documented tolerance to <1000 mg/day. As outlined in Table 243, there are many forms of tolerance, likely arising via multiple mechanisms.
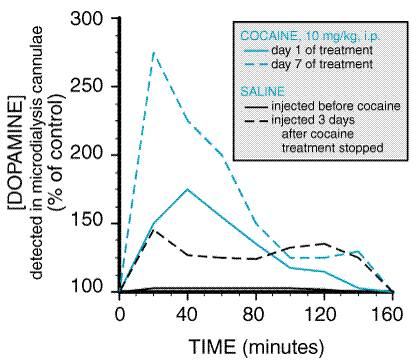
Tolerance develops to some drug effects much more rapidly than to other effects of the same drug. For example, tolerance develops rapidly to the euphoria produced by opioids such as heroin, and addicts tend to increase their dose in order to reexperience that elusive 'high.' In contrast, tolerance to the gastrointestinal effects of opiates develops more slowly. The discrepancy between tolerance to euphorigenic effects and tolerance to effects on vital functions, such as respiration and blood pressure, can lead to potentially fatal accidents in sedative abusers. Innate tolerance refers to genetically determined sensitivity (or lack of sensitivity) to a drug that is observed the first time that the drug is administered. Innate tolerance is discussed above as a host variable that influences the development of abuse or addiction. Acquired tolerance can be divided into three types: pharmacokinetic, pharmacodynamic, and learned tolerance, including a form of behavioral tolerance referred to as conditioned tolerance. Pharmacokinetic or dispositional tolerance refers to changes in the distribution or metabolism of the drug after repeated drug administration, such that reduced concentrations are present in the blood and subsequently at the sites of drug action (see Chapter 1: Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, and Elimination). The most common mechanism is an increase in the rate of metabolism of the drug. For example, barbiturates stimulate the production of higher levels of hepatic microsomal enzymes, causing more rapid removal and breakdown of barbiturates from the circulation. Since the same enzymes metabolize many other drugs, they too are metabolized more quickly. This results in a decrease in their plasma levels as well and thus a reduction in their effects. Pharmacodynamic tolerance refers to adaptive changes that have taken place within systems affected by the drug, so that response to a given concentration of the drug is reduced. Examples include drug-induced changes in receptor density or efficiency of receptor coupling to signal transduction pathways (see Chapter 2: Pharmacodynamics: Mechanisms of Drug Action and the Relationship Between Drug Concentration and Effect). Learned tolerance refers to a reduction in the effects of a drug due to compensatory mechanisms that are learned. One type of learned tolerance is called behavioral tolerance. This simply describes the skills that can be developed through repeated experiences with attempting to function despite a state of mild to moderate intoxication. A common example is learning to walk a straight line in spite of the motor impairment produced by alcohol intoxication. This probably involves both acquisition of motor skills and the learned awareness of one's deficit, causing the person to walk more carefully. At higher levels of intoxication, behavioral tolerance is overcome, and the deficits are obvious. A special case of behavioral tolerance is referred to as conditioned tolerance. Conditioned tolerance (situation-specific tolerance) is a learning mechanism that develops when environmental cues such as sights, smells, or situations consistently are paired with the administration of a drug. When a drug affects homeostatic balance by producing sedation and changes in blood pressure, pulse rate, gut activity, etc., there is usually a reflexive counteraction or adaptation that attempts to maintain the status quo. If a drug always is taken in the presence of specific environmental cues (smell of drug preparation, sight of syringe), these cues begin to predict the appearance of the drug. Then the adaptations begin to occur even before the drug reaches its sites of action. If the drug always is preceded by the same cues, the adaptive response to the drug will be learned, and this will prevent the full manifestation of the drug's effects (tolerance). This mechanism of conditioned tolerance production follows classical (Pavlovian) principles of learning and results in drug tolerance being evident under circumstances where the drug is 'expected.' When the drug is received under novel or 'unexpected' circumstances, tolerance is reduced and drug effects are enhanced (Wikler, 1973; Siegel 1976). The term acute tolerance refers to rapid tolerance developing with repeated use on a single occasion such as in a 'binge.' For example, cocaine often is used in a binge, with repeated doses over one to several hours, sometimes longer. Under binge dosing, there will be a decrease in response to subsequent doses of cocaine during the binge. This is the opposite of sensitization, observed with an intermittent dosing schedule, described below. Sensitization With stimulants such as cocaine or amphetamine, reverse tolerance or sensitization can occur. This refers to an increase in response with repetition of the same dose of the drug. Sensitization results in a shift to the left of the doseresponse curve, as illustrated schematically in Figure 241. For example, with repeated daily administration to rats of a dose of cocaine that produces increased motor activity, the effect increases over several days, even though the dose remains constant. A conditioned response also can be a part of sensitization to cocaine. Simply putting a rat into a cage where cocaine is expected or giving a placebo injection after several days of receiving cocaine under the same circumstances produces an increase in motor activity as though cocaine actually were giveni.e., a conditioned response. Sensitization, in contrast to acute tolerance during a binge, requires a longer interval between doses, usually about a day. Sensitization has been studied in rats equipped with microdialysis cannulae for monitoring extracellular dopamine (Kalivas and Duffy, 1990; see Figure 242). The initial response to 10 mg/kg of cocaine administered intraperitoneally is an increase in measured dopamine levels. After seven daily injections, the dopamine increase is significantly greater than on the first day, and the behavioral response also is greater. Figure 242 also provides an example of a conditioned response (learned drug effect), since injection of saline produced both an increase in dopamine levels and an increase in behavioral activity when it was administered 3 days after cocaine injections had stopped. Little research on sensitization has been conducted in human subjects, but the results suggest that the phenomenon can occur. It has been postulated that stimulant psychosis results from a sensitized response after long periods of use.
Cross-Tolerance Cross-tolerance refers to the fact that repeated use of drugs in a given category confers tolerance not only to the drug being used but also to other drugs in the same structural and mechanistic category. Understanding cross-tolerance is important in the medical management of persons dependent on any drug. Detoxification is a form of treatment for drug dependence that involves giving gradually decreasing doses of the drug to prevent withdrawal symptoms, thereby weaning the patient from the drug of dependence (see below). Detoxification can be accomplished with any medication that produces cross-tolerance to the initial drug of dependence. For example, users of heroin also are tolerant to other opioids. Thus the detoxification of heroin-dependent patients can be accomplished with any medication that activates opiate receptors (opioid drug; see Chapter 23: Opioid Analgesics). Physical Dependence Physical dependence is a state that develops as a result of the adaptation (tolerance) produced by a resetting of homeostatic mechanisms in response to repeated drug use. Drugs can affect numerous systems that previously were in equilibrium; these systems must find a new balance in the presence of inhibition or stimulation by a specific drug. A person in this adapted or physically dependent state requires continued administration of the drug to maintain normal function. If administration of the drug is stopped abruptly, there is another imbalance, and the affected systems must again go through a process of readjusting to a new equilibrium without the drug. Withdrawal Syndrome The appearance of a withdrawal syndrome when administration of the drug is terminated is the only actual evidence of physical dependence. Withdrawal signs and symptoms occur when drug administration in a physically dependent person is abruptly terminated. Withdrawal symptoms have at least two origins: (1) removal of the drug of dependence, and (2) central nervous system hyperarousal due to readaptation to the absence of the drug of dependence. Pharmacokinetic variables are of considerable importance in the amplitude and duration of the withdrawal syndrome. Withdrawal symptoms are characteristic for a given category of drugs, and they tend to be opposite to the original effects produced by the drug before tolerance developed. Thus, a drug (such as an opioid agonist) that produces meiotic (constricted) pupils and slow heart rate will result in dilated pupils and tachycardia when it is withdrawn from a dependent person. Tolerance, physical dependence, and withdrawal are all biological
phenomena. They are the natural consequences of drug use. They can be
produced in experimental animals and in any human being who takes certain
medications repeatedly. These symptoms in themselves do not imply that the
individual is involved in abuse or addiction. Patients who take medicine
for appropriate medical indications and in the correct dose still may show
tolerance, physical dependence, and withdrawal symptoms if the drug is
stopped abruptly rather than gradually. For example, a hypertensive
patient receiving a 'Medical addict' is a term used to describe a patient in treatment for a medical disorder who has become 'addicted' to the available prescribed drugs; the patient begins taking them in excessive doses, out of control. An example would be a patient with chronic pain, anxiety, or insomnia who begins using the prescribed medication more often than directed by the physician. If the physician restricts the prescriptions, the patient may begin seeing several doctors without the knowledge of the primary physician. Such patients also may visit emergency rooms for the purpose of obtaining additional medication. This scenario rarely occurs, considering the large number of patients who receive medications capable of producing tolerance and physical dependence. Fear of producing such medical addicts results in needless suffering among patients with pain, as physicians needlessly limit appropriate medications. Tolerance and physical dependence are inevitable consequences of chronic treatment with opioids and certain other drugs, but tolerance and physical dependence, by themselves, do not imply 'addiction.' |
Clinical Issues
|
The treatment of physically dependent individuals is discussed below with reference to the specific drug of abuse and dependence problems characteristic to each category: central nervous system (CNS) depressants, including alcohol and sedatives; nicotine and tobacco; opioids; psychostimulants, such as amphetamine and cocaine; cannabinolds; psychedelic drugs; and inhalants (volatile solvents, nitrous oxide, ethyl ether). Abuse of combinations of drugs across these categories is common. Alcohol is such a widely available drug that it is combined with practically all other categories. Some combinations reportedly are taken because of their interactive effects. An example is the combination of heroin and cocaine ('speedball'), which is described with the opioid category. When confronted with a patient exhibiting signs of overdose or withdrawal, the physician must be aware of these possible combinations, because each drug may require specific treatment. Central Nervous System Depressants Ethanol The use of ethyl alcohol prepared from the fermentation of sugars, starches, or other carbohydrates dates back as early as recorded history. Experimentation with ethanol is almost universal, and a high proportion of users find the experience pleasant. Approximately 70% of American adults occasionally consume ethanol (commonly called alcohol), and the lifetime prevalence of alcohol abuse and alcohol addiction (alcoholism) in this society is 5% to 10% for men and 3% to 5% for women. Ethanol is classed as a depressant because it indeed produces sedation and sleep. However, the initial effects of alcohol, particularly at lower doses, often are perceived as stimulation due to a suppression of inhibitory systems (see Chapter 18: Ethanol). Those who perceive only sedation from alcohol tend to choose not to drink when evaluated in a test procedure (de Wit et al., 1989). Alcohol impairs recent memory and, in high doses, produces the phenomenon of 'blackouts,' after which the drinker has no memory of his or her behavior while intoxicated. The effects of alcohol on memory are unclear (Mello, 1973), but evidence suggests that reports from patients about their reasons for drinking and their behavior during a binge are not reliable. Alcohol-dependent persons often say that they drink to relieve anxiety or depression. When allowed to drink under observation, however, alcoholics typically become more dysphoric as drinking continues (Mendelson and Mello, 1979), thus contradicting the tension-reduction explanation. Tolerance, Physical Dependence, and Withdrawal Mild intoxication by alcohol is familiar to almost everyone, but the symptoms vary among individuals. Some simply experience motor incoordination and sleepiness. Others initially become stimulated and garrulous. As the blood level increases, the sedating effects increase, with eventual coma and death at high alcohol levels. The initial sensitivity (innate tolerance) to alcohol varies greatly among individuals and is related to family history of alcoholism (Schuckit and Smith, 1997). Experience with alcohol can produce greater tolerance (acquired tolerance), such that extremely high blood levels (300 to 400 mg/dl) can be found in alcoholics who do not appear grossly sedated. In these cases, the lethal dose does not increase proportionately to the sedating dose, and thus the margin of safety (therapeutic index) is decreased. Heavy consumers of alcohol not only acquire tolerance but also inevitably develop a state of physical dependence. This often leads to drinking in the morning to restore blood alcohol levels diminished during the night. Eventually they may awaken during the night and take a drink to avoid the restlessness produced by falling alcohol levels. The alcohol withdrawal syndrome (Table 244) generally depends on the size of the average daily dose and usually is 'treated' by resumption of alcohol ingestion. Withdrawal symptoms are experienced frequently, but they usually are not severe or life threatening until they occur in conjunction with other problems, such as infection, trauma, malnutrition, or electrolyte imbalance. In the setting of such complications, the syndrome of delirium tremens becomes likely (see Table 244). Alcohol produces cross-tolerance to other sedatives such as benzodiazepines. This tolerance is operative in abstinent alcoholics, but while the alcoholic is drinking, the sedating effects of alcohol add to those of other drugs, making the combination more dangerous. This is particularly true for benzodiazepines, which are relatively safe in overdose when given alone but potentially are lethal in combination with alcohol. The chronic use of alcohol as well as that of other sedatives is associated with the development of depression (McLellan et al., 1979), and the risk of suicide among alcoholics is one of the highest of any diagnostic category. Cognitive deficits have been reported in alcoholics tested while sober. These deficits usually improve after weeks to months of abstinence (Grant, 1987). More severe recent memory impairment is associated with specific brain damage caused by nutritional deficiencies, which are common in alcoholics. Alcohol is toxic to many organ systems. As a result, the medical complications of alcohol abuse and dependence include liver disease, cardiovascular disease, endocrine and gastrointestinal effects, and malnutrition, in addition to the CNS dysfunctions outlined above (see Chapter 18: Ethanol). Ethanol readily crosses the placental barrier, producing the fetal alcohol syndrome, a major cause of mental retardation (see Chapter 18: Ethanol). Pharmacological Interventions Detoxification A patient who presents in a medical setting with an alcohol-withdrawal syndrome should be considered to have a potentially lethal condition. Although most mild cases of alcohol withdrawal never come to medical attention, severe cases require general evaluation; attention to hydration and electrolytes; vitamins, especially high-dose thiamine; and a sedating medication that has cross-tolerance with alcohol. A short-acting benzodiazepine such as oxazepam can be given at doses sufficient to block or diminish the symptoms described in Table 244; some authorities recommend a long-acting benzodiazepine unless there is demonstrated liver impairment. Anticonvulsants such as carbamazepine have been shown to be effective in alcohol withdrawal, although they appear not to relieve subjective symptoms as well as benzodiazepines. After medical evaluation, uncomplicated alcohol withdrawal can be treated effectively on an outpatient basis (Hayashida et al., 1989). When there are medical problems or a history of seizures, hospitalization is required. Other Measures Detoxification is only the first step of treatment. Complete abstinence is the objective of long-term treatment, and this is accomplished mainly by behavioral approaches. Medications that aid in this process are being sought. Disulfiram (see Chapter 18: Ethanol) has been useful in some programs that focus behavioral efforts on the ingestion of the medication. Disulfiram blocks the metabolism of alcohol, resulting in the accumulation of acetaldehyde, which produces an unpleasant flushing reaction when alcohol is ingested. Knowledge of this unpleasant reaction helps the patient resist taking a drink. Although quite effective pharmacologically, disulfiram has not been found to be effective in controlled clinical trials, because so many patients failed to ingest the medication. Another FDA-approved medication used as an adjunct in the treatment of alcoholism is naltrexone (see Chapter 18: Ethanol). This opiate receptor antagonist appears to block some of the reinforcing properties of alcohol and has resulted in a decreased rate of relapse to alcohol drinking in several double-blind clinical trials. It works best in combination with behavioral treatment programs that encourage adherence to medication and to remaining abstinent from alcohol. Benzodiazepines and Other Nonalcohol Sedatives Benzodiazepines are among the most commonly prescribed drugs worldwide; they are used mainly for the treatment of anxiety disorders and insomnia (Chapters 17: Hypnotics and Sedatives and 19: Drugs and the Treatment of Psychiatric Disorders: Depression and Anxiety Disorders). Considering their widespread use, intentional abuse of prescription benzodiazepines is relatively rare. When a benzodiazepine is taken for up to several weeks, there is little tolerance and no difficulty in stopping the medication when the condition no longer warrants its use. After several months, the proportion of patients who become tolerant increases, and reducing the dose or stopping the medication produces withdrawal symptoms (Table 245). It can be difficult to distinguish withdrawal symptoms from the reappearance of the anxiety symptoms that caused the benzodiazepine to be prescribed initially. Some patients may increase their dose over time, because tolerance definitely develops to the sedative effects. Many patients and their physicians, however, contend that antianxiety benefits continue to occur long after tolerance to the sedating effects. Moreover, these patients continue to take the medication for years according to medical directions without increasing their dose and are able to function very effectively as long as they take the benzodiazepine. The degree to which tolerance develops to the anxiolytic effects of benzodiazepines is a subject of controversy (Lader and File, 1987). There is, however, good evidence that significant tolerance does not develop to all benzodiazepine actions, because some effects of acute doses on memory persist in patients who have taken benzodiazepines for years (Lucki et al., 1986). The American Psychiatric Association formed a task force that reviewed the issues and published guidelines on the proper medical use of benzodiazepines (American Psychiatric Association, 1990). Intermittent use when symptoms occur retards the development of tolerance and is, therefore, preferable to daily use. Patients with a history of alcohol or other drug abuse problems have an increased risk for the development of benzodiazepine abuse and should rarely, if ever, be treated with benzodiazepines on a chronic basis. While relatively few patients who receive benzodiazepines for medical indications abuse their medication, there are individuals who specifically seek benzodiazepines for their ability to produce a 'high.' Among these abusers, there are differences in drug popularity, with those benzodiazepines that have a rapid onset, such as diazepam and alprazolam, tending to be the most desirable. The drugs may be obtained by simulating a medical condition and deceiving physicians or simply through illicit channels. Street drug dealers provide benzodiazepines in most major cities at a relatively low cost. Such unsupervised use can lead to the self-administration of huge quantities of such drugs and therefore tolerance to the benzodiazepine's sedating effects. For example, while 5 to 20 mg/day of diazepam is a typical dose for a patient receiving prescribed medication, abusers may take over 1000 mg/day and not appear grossly sedated. Abusers may combine benzodiazepines with other drugs to increase the effect. For example, it is part of the 'street lore' that taking diazepam 30 minutes after an oral dose of methadone will produce an augmented high that is not obtainable with either drug alone. While there is some illicit use of benzodiazepines as a primary drug of abuse, most of the nonsupervised use seems to be by abusers of other drugs who are attempting to self-medicate the side effects or withdrawal effects of their primary drug of abuse. Thus, cocaine addicts often take diazepam to relieve the irritability and agitation produced by cocaine binges, and opioid addicts find that diazepam and other benzodiazepines relieve some of the anxiety symptoms of opioid withdrawal when they are unable to obtain their preferred drug. Pharmacological Interventions If patients receiving long-term benzodiazepine treatment by prescription wish to stop their medication, the process may take months of gradual dose reduction. Symptoms as listed in Table 245 may occur during this outpatient detoxification, but in most cases the symptoms are mild. If anxiety symptoms return, a nonbenzodiazepine such as buspirone may be prescribed, but this agent usually is less effective than benzodiazepines for treatment of anxiety in these patients. Some authorities recommend transferring the patient to a long-half-life benzodiazepine during detoxification; other medications recommended include the anticonvulsants carbamazepine and phenobarbital. Controlled studies comparing different treatment regimens are lacking. Since patients who have been on low doses of benzodiazepines for years usually have no adverse effects, the physician and patient should jointly decide whether detoxification and possible transfer to a new anxiolytic is worth the effort. The specific benzodiazepine receptor antagonist flumazenil has been found useful in the treatment of overdose and in reversing the effects of long-acting benzodiazepines used in anesthesia (see Chapter 17: Hypnotics and Sedatives). It has been tried in the treatment of persistent withdrawal symptoms after cessation of long-term benzodiazepine treatment. Deliberate abusers of high doses of benzodiazepines usually require inpatient detoxification. Frequently, benzodiazepine abuse is part of a combined dependence involving alcohol, opioids, and cocaine. Detoxification can be a complex clinical pharmacological problem, requiring knowledge of the pharmacokinetics of each drug. The patient's history may not be reliable, not simply because of lying but also because the patient frequently does not know the true identity of drugs purchased on the street. Medication for detoxification should not be prescribed by the 'cookbook' approach but by careful titration and patient observation. The withdrawal syndrome from diazepam, for example, may not become evident until the patient develops a seizure in the second week of hospitalization. One approach to complex detoxification is to focus on the CNS-depressant drug and temporarily hold the opioid component constant with a low dose of methadone. Opioid detoxification can begin later. A long-acting benzodiazepine, such as diazepam or clorazepate, or a long-acting barbiturate, such as phenobarbital, can be used to block the sedative withdrawal symptoms. The phenobarbital dose should be determined by a series of test doses and subsequent observations to determine the level of tolerance. Most complex detoxifications can be accomplished using this phenobarbital loading-dose strategy (see Robinson et al., 1981). After detoxification, the prevention of relapse requires a long-term outpatient rehabilitation program similar to that for the treatment of alcoholism. No specific medications have been found to be useful in the rehabilitation of sedative abusersbut, of course, specific psychiatric disorders such as depression or schizophrenia, if present, require appropriate medications. Barbiturates and Nonbenzodiazepine Sedatives The use of barbiturates and other nonbenzodiazepine sedating medications has declined greatly in recent years due to the increased safety and efficacy of the newer medications. Abuse problems with barbiturates resemble those seen with benzodiazepines in many ways. Treatment of abuse and addiction should be handled similarly to interventions for the abuse of alcohol and benzodiazepines. Because drugs in this category frequently are prescribed as hypnotics for patients complaining of insomnia, the physician should be aware of the problems that can develop when the hypnotic agent is withdrawn. Insomnia rarely should be treated with medication as a primary disorder except when produced by short-term stressful situations. Insomnia often is a symptom of an underlying chronic problem, such as depression, or may be due simply to a change in sleep requirements with age. Prescription of sedative medications, however, can change the physiology of sleep, with subsequent tolerance to these medication effects. When the sedative is stopped, there is a rebound effect (Kales et al., 1979). This medication-induced insomnia requires detoxification by gradual dose reduction. Nicotine The basic pharmacology of nicotine is discussed in Chapter 9: Agents
Acting at the Neuromuscular Junction and Autonomic Ganglia. Nicotine has
complex effects that result in its self-administration. Because nicotine
provides the reinforcement for the smoking of cigarettes, the most common
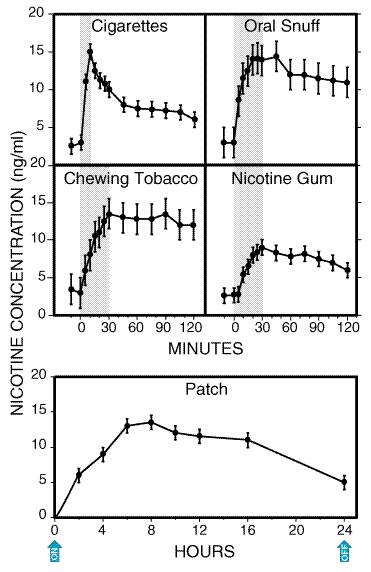
cause of preventable death and disease in the Cigarette (nicotine) addiction is influenced by multiple variables. Nicotine itself produces reinforcement; users compare nicotine to stimulants such as cocaine or amphetamine, although its effects are of lower magnitude. While there are many casual users of alcohol and cocaine, few individuals who smoke cigarettes smoke a small enough quantity (five cigarettes or fewer per day) to avoid dependence. Nicotine is absorbed readily through the skin, mucous membranes, and, of course, the lungs. The pulmonary route produces discernible CNS effects in as little as seven seconds. Thus, each puff produces some discrete reinforcement. With 10 puffs per cigarette, the one-pack-per-day smoker reinforces the habit 200 times daily. The timing, setting, situation, and preparation all become associated repetitively with the effects of nicotine. Nicotine has both stimulant and depressant actions. The smoker feels alert, yet there is some muscle relaxation. Nicotine activates the nucleus accumbens reward system in the brain, discussed earlier; increased extracellular dopamine has been found in this region after nicotine injections in rats. Nicotine affects other systems as well, including the release of endogenous opioids and glucocorticoids. There is evidence for tolerance to the subjective effects of nicotine. Smokers typically report that the first cigarette of the day after a night of abstinence gives the 'best' feeling. Smokers who return to cigarettes after a period of abstinence may experience nausea if they return immediately to their previous dose. Persons naive to the effects of nicotine will experience nausea at low nicotine blood levels, and smokers will experience nausea if nicotine levels are raised above their accustomed levels. Negative reinforcement refers to the benefits obtained from the termination of an unpleasant state. In dependent smokers, there is evidence that the urge to smoke correlates with a low nicotine blood level, as though smoking were a means to achieve a certain nicotine level and thus avoid withdrawal symptoms. Some smokers even awaken during the night to have a cigarette, which ameliorates the effect of low nicotine blood levels that could disrupt sleep. If the nicotine level is maintained artificially by a slow intravenous infusion, there is a decrease in the number of cigarettes smoked and in the number of puffs (Russell, 1987). Thus, smokers may be smoking to achieve the reward of nicotine effects, to avoid the pain of nicotine withdrawal or, most likely, a combination of the two. Nicotine withdrawal symptoms are listed in Table 246. Depressed mood (dysthymic disorder, affective disorder) is associated with nicotine dependence, but it is not known whether depression predisposes one to begin smoking or depression develops during the course of nicotine dependence. Depression significantly increases during smoking withdrawal, and this is cited as one reason for relapse. Pharmacological Interventions The nicotine withdrawal syndrome can be alleviated by nicotine replacement therapy, available without a prescription. Figure 243 shows the blood nicotine concentrations achieved by different methods of nicotine delivery. Because nicotine gum and a nicotine patch do not achieve the peak levels seen with cigarettes, they do not produce the same magnitude of subjective effects as nicotine. These methods do, however, suppress the symptoms of nicotine withdrawal. Thus, smokers should be able to transfer their dependence to the alternative delivery system and gradually reduce the daily nicotine dose with minimal symptoms. Although this results in more smokers achieving abstinence, most resume smoking over the ensuing weeks or months. Comparisons with placebo treatment show large benefits of nicotine replacement at six weeks, but the effect diminishes with time. The nicotine patch produces a steady blood level (Figure 243) and seems to have better patient compliance than that observed with nicotine gum. Verified abstinence rates at 12 months are reported to be in the range of 20%, which is worse than the success rate for any other addiction. The goal of complete abstinence rather than significant reduction is necessary for success; when ex-smokers 'slip' and begin smoking a little, they usually relapse quickly to their prior level of dependence. Bupropion, an antidepressant (see Chapter 19: Drugs and the Treatment of Psychiatric Disorders: Depression and Anxiety Disorders), has been found to improve abstinence rates among smokers. Some smokers report that it reduces their craving for cigarettes, and controlled studies show reduced relapse in smokers randomized to this medication. The best results are in smokers receiving both nicotine patch and bupropion. Behavioral treatment in combination with medication is considered the treatment of choice.
Opioids Opioid drugs are used primarily for the treatment of pain (see Chapter 23: Opioid Analgesics). Some of the CNS mechanisms that reduce the perception of pain also produce a state of well-being or euphoria. Thus, opioid drugs also are taken outside of medical channels for the purpose of obtaining the effects on mood. This potential for abuse has generated much research on separating the mechanism of analgesia from that of euphoria in the hope of eventually developing a potent analgesic that does not activate brain reward systems. Although this research has led to advances in understanding the physiology of pain, the standard medications for severe pain remain the derivatives of the opium poppy (opiates) and synthetic drugs that activate the same receptors (opioids). Drugs modeled after the endogenous opioid peptides may one day provide more specific treatment, but none of these currently is available for clinical use. Medications that do not act at opiate receptors, such as the nonsteroidal antiinflammatory drugs, have an important role in certain types of pain, especially chronic pain; but for acute pain and for severe chronic pain, the opioid drugs are the most effective. A recent development in pain control stems from a greater
understanding of the mechanism of tolerance to 'mu' ( The subjective effects of opioid drugs are useful in the management of acute pain. This is particularly true in high-anxiety situations, such as the crushing chest pain of a myocardial infarction, when the relaxing, anxiolytic effects complement the analgesia. Normal volunteers with no pain given opioids in the laboratory may report the effects as unpleasant because of the side effects, such as nausea, vomiting, and sedation. Patients with pain rarely develop abuse or addiction problems. Of course, patients receiving opioids develop tolerance routinely, and if the medication is stopped abruptly, they will show the signs of an opioid withdrawal syndrome, the evidence for physical dependence. Opioids should never be withheld from patients with cancer out of fear of producing addiction. If chronic opioid medication is indicated, it is preferable to prescribe an orally active, slow-onset opioid with a long duration of action. These qualities reduce the likelihood of producing euphoria at onset of withdrawal symptoms as the medication wears off. Methadone is an excellent choice for the management of chronic severe pain. Controlled-release, oral morphine (MS CONTIN, others) or controlled-release oxycodone (OXYCONTIN) are other possibilities. Rapid-onset, short-duration opioids are excellent for acute, short-term use, such as during the postoperative period. As tolerance and physical dependence develop, however, the patient may experience the early symptoms of withdrawal between doses, and during withdrawal, the threshold for pain decreases. Thus, for chronic administration, the long-acting opioids are recommended. The major risk for abuse or addiction occurs in patients complaining of pain with no clear physical explanation or with evidence of a chronic disorder that is not life-threatening. Examples are chronic headaches, backaches, abdominal pain, or peripheral neuropathy. Even in these cases, an opioid might be considered as a brief emergency treatment, but long-term treatment with opioids should be used only after other alternatives have been exhausted. In those relatively rare patients who develop abuse, the transition from legitimate use to abuse often begins with patients returning to their physician earlier than scheduled to get a new prescription or visiting emergency rooms of different hospitals complaining of acute pain and asking for an opioid injection. Heroin is
the most important opioid drug that is abused. There is no legal supply of
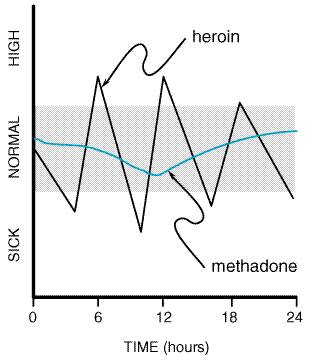
heroin for clinical use in the There is no accurate way to count the number of heroin addicts, but based on extrapolation from overdose deaths, number of applicants for treatment, and number of heroin addicts arrested, the estimates range from 800,000 to 1 million. In national surveys, approximately three adults report having tried heroin for every one who became addicted to the drug. Tolerance, Dependence, and Withdrawal Injection of a heroin solution produces a variety of sensations described as warmth, taste, or high and intense pleasure ('rush') often compared to sexual orgasm. There are some differences among the opioids in their acute effects, with morphine producing more of a histamine-releasing effect and meperidine producing more excitation or confusion. Even experienced opioid addicts, however, cannot distinguish between heroin and hydromorphone in double-blind tests. Thus, the popularity of heroin may be due to its availability on the illicit market and its rapid onset. After intravenous injection, the effects begin in less than a minute. Heroin has high lipid solubility, crosses the blood-brain barrier quickly, and is deacetylated to the active metabolites, 6-monoacetyl morphine and morphine. After the intense euphoria, which lasts from 45 seconds to several minutes, there is a period of sedation and tranquillity ('on the nod') lasting up to an hour. The effects of heroin wear off in 3 to 5 hours, depending on the dose. Experienced users may inject two to four times per day. Thus, the heroin addict is constantly oscillating between being 'high' and feeling the sickness of early withdrawal (Figure 244). This produces many problems in the homeostatic systems regulated, at least in part, by endogenous opioids. For example, the hypothalamic-pituitary-gonadal axis and the hypothalamic-pituitary-adrenal axis are abnormal in heroin addicts. Women on heroin have irregular menses, and men have a variety of sexual performance problems. Mood also is affected. Heroin addicts are relatively docile and compliant after taking heroin, but during withdrawal, they become irritable and aggressive.
Based on patient reports, tolerance develops early to the euphoria-producing effects of opioids. There also is tolerance to the respiratory depressant, analgesic, sedative, and emetic properties. Heroin users tend to increase their daily dose, depending on their financial resources and the availability of the drug. If a supply is available, the dose can be progressively increased 100-fold. Even in highly tolerant individuals, the possibility of overdose remains if tolerance is exceeded. Overdose is likely to occur when potency of the street sample is unexpectedly high or when the heroin is mixed with a far more potent opioid, such as fentanyl, synthesized in clandestine laboratories. Addiction to heroin or other short-acting opioids produces behavioral disruptions and usually becomes incompatible with a productive life. There is a significant risk for opioid abuse and dependence among physicians and other health-care workers who have access to potent opioids, thus enabling unsupervised experimentation. Physicians often begin by assuming that they can manage their own dose, and they may rationalize their behavior based on the beneficial effects of the drug. Over time, however, the typical unsupervised opioid user loses control, and behavioral changes are observed by family and coworkers. Apart from the behavioral changes and the risk of overdose, especially with very potent opioids, chronic use of opioids is relatively nontoxic. Opioids frequently are used in combinations with other drugs. A common combination is heroin and cocaine ('speedball'). Users report an improved euphoria because of the combination, and there is evidence of an interaction, because the partial opioid agonist buprenorphine reduces cocaine self-administration in animals (Mello et al., 1989). Cocaine reduces the signs of opioid withdrawal (Kosten, 1990), and heroin may reduce the irritability seen in chronic cocaine users. The mortality rate for street heroin users is very high. Early death comes from involvement in crime to support the habit; from uncertainty about the dose, the purity, and even the identity of what is purchased on the street; and from serious infections associated with unsterile drugs and sharing of injection paraphernalia. Heroin users commonly acquire bacterial infections producing skin abscesses, endocarditis, pulmonary infections, especially tuberculosis, and viral infections producing hepatitis and acquired immunodeficiency syndrome (AIDS). As with other addictions, the first stage of treatment addresses physical dependence and consists of detoxification. The opioid withdrawal syndrome (Table 247) is very unpleasant but not life-threatening. It begins within 6 to 12 hours after the last dose of a short-acting opioid and as long as 72 to 84 hours after a very long-acting opioid medication. Heroin addicts go through early stages of this syndrome frequently when heroin is scarce or expensive. Some therapeutic communities, as a matter of policy, elect not to treat withdrawal so that the addict can experience the suffering while being given group support. The duration and intensity of the syndrome are related to the clearance of the individual drug. Heroin withdrawal is brief (5 to 10 days) and intense. Methadone withdrawal is slower in onset and lasts longer. Protracted withdrawal also is likely to be longer with methadone. (See more detailed discussions of protracted withdrawal under 'Long-Term Management,' below.) Pharmacological Interventions Opioid withdrawal signs and symptoms can be treated by three different approaches. The first and most commonly used depends on cross-tolerance and consists of transfer to a prescription opioid medication and then gradual dose reduction. The same principles of detoxification apply as for other types of physical dependence. It is convenient to change the patient from a short-acting opioid such as heroin to a long-acting one such as methadone. The initial dose of methadone is typically 20 to 30 mg. This is a test dose to determine the level needed to reduce observed withdrawal symptoms. The first day's total dose then can be calculated depending on the response and then reduced by 20% per day during the course of detoxification. A second approach to detoxification involves the use of clonidine,
a medication approved only for the treatment of hypertension (see Chapter
33: Antihypertensive Agents and the Drug Therapy of Hypertension). Clonidine
is an A third method of treating opioid withdrawal involves activation of the endogenous opioid system without medication. The techniques proposed include acupuncture and several methods of CNS activation utilizing transcutaneous electrical stimulation. While theoretically attractive, this has not yet been found to be practical. Rapid antagonist-precipitated opioid detoxification under general anesthesia has received considerable publicity, because it promises detoxification in several hours while the patient is unconscious and thus not experiencing withdrawal discomfort. A mixture of medications has been used, and morbidity and mortality as reported in the lay press are unacceptable, with no demonstrated advantage in long-term outcome. Long-Term Management If patients are simply discharged from the hospital after withdrawal from opioids, there is a high probability of a quick return to compulsive opioid use. Addiction is a chronic disorder that requires long-term treatment. There are numerous factors that influence relapse. One factor is that the withdrawal syndrome does not end in 5 to 7 days. There are subtle signs and symptoms often called the protracted withdrawal syndrome (Table 247) that persist for up to 6 months. Physiological measures tend to oscillate as though a new set point were being established (Martin and Jasinski, 1969); during this phase, outpatient drug-free treatment has a low probability of success, even when the patient has received intensive prior treatment while protected from relapse in a residential program. The most successful treatment for heroin addiction consists of stabilization on methadone. Patients who repeatedly relapse during drug-free treatment can be transferred directly to methadone without requiring detoxification. The dose of methadone must be sufficient to prevent withdrawal symptoms for at least 24 hours. Levomethadyl acetate hydrochloride (ORLAAM) is another maintenance option that will block withdrawal for 72 hours. Agonist Maintenance Patients receiving methadone or levomethadyl acetate will not experience the ups and downs they experienced while on heroin (Figure 244). Drug craving diminishes and may disappear. Neuroendocrine rhythms eventually are restored (Kreek, 1992). Because of cross-tolerance (from methadone to heroin), patients who inject street heroin report a reduced effect from usual heroin doses. This cross-tolerance effect is dose-related, so that higher methadone maintenance doses result in less illicit opioid use as determined by random urine testing. Patients become tolerant to the sedating effects of methadone and become able to attend school or function in a job. Opioids also have a persistent, mild, stimulating effect noticeable after tolerance to the sedating effect, such that reaction time is quicker and vigilance is increased on a stable dose of methadone. Antagonist Treatment Another pharmacological option is opioid antagonist treatment. Naltrexone
(see Chapter 23: Opioid Analgesics) is an antagonist with a high
affinity for the New Treatment Options Two important advances in the treatment of opioid addiction are
currently in clinical trials. Buprenorphine, a partial agonist at Cocaine and Other Psychostimulants Cocaine More than 23 million Americans are estimated to have used cocaine at some time, but the number of current users declined from an estimated 8.6 million occasional users and 5.8 million regular users to 3.6 million who still identified themselves as sometimes using cocaine in 1995. The number of frequent users (at least weekly) has remained steady since 1991 at about 640,000 persons. Not all users become addicts, and the variables that influence this risk are discussed at the beginning of this chapter. A key factor is the widespread availability of relatively inexpensive cocaine in the alkaloidal (free base, 'crack') form suitable for smoking and the hydrochloride powder form suitable for nasal or intravenous use. Drug abuse in men occurs about twice as frequently as in women. However, smoked cocaine use is particularly common in young women of childbearing age, who may use cocaine in this manner as commonly as do men. The reinforcing effects of cocaine and cocaine analogs correlate best with their effectiveness in blocking the transporter that recovers dopamine from the synapse. This leads to increased dopaminergic stimulation at critical brain sites (Ritz et al., 1987). However, cocaine also blocks both norepinephrine (NE) and serotonin (5-HT) reuptake, and chronic use of cocaine produces changes in these neurotransmitter systems as measured by reductions in the neurotransmitter metabolites MHPG (3-methoxy-4-hydroxyphenethyleneglycol) and 5-HIAA (5-hydroxyindoleacetic acid). The general pharmacology and legitimate use of cocaine are discussed in Chapter 15: Local Anesthetics. Cocaine produces a dose-dependent increase in heart rate and blood pressure accompanied by increased arousal, improved performance on tasks of vigilance and alertness, and a sense of self-confidence and well-being. Higher doses produce euphoria, which has a brief duration and often is followed by a desire for more drug. Involuntary motor activity, stereotyped behavior, and paranoia may occur after repeated doses. Irritability and increased risk of violence are found among heavy chronic users. The half-life of cocaine in plasma is about 50 minutes, but inhalant (crack) users typically desire more cocaine after 10 to 30 minutes. Intranasal and intravenous uses also result in a 'high' of shorter duration than would be predicted by plasma cocaine levels, suggesting that a declining plasma concentration is associated with termination of the high and resumption of cocaine seeking. This theory is supported by positron emission tomography imaging studies using C11-labeled cocaine, which show that the time course of subjective euphoria parallels the uptake and displacement of the drug in the corpus striatum (Volkow et al., 1999). Addiction is the most common complication of cocaine use. Some users, especially intranasal users, can continue intermittent use for years. Others become compulsive users despite elaborate methods to maintain control. Stimulants tend to be used much more irregularly than opioids, nicotine, and alcohol. Binge use is very common, and a binge may last hours to days, terminating only when supplies of the drug are exhausted. The major route for cocaine metabolism involves hydrolysis of each of its two ester groups. Benzoylecgonine, produced upon loss of the methyl group, represents the major urinary metabolite and can be found in the urine for 2 to 5 days after a binge. As a result, benzoylecgonine tests are useful for detecting cocaine use; heavy users have been found to have detectable amounts of the metabolite in urine for up to 10 days following a binge. Cocaine frequently is used in combination with other drugs. The cocaine-heroin combination is discussed above, with opioids. Alcohol is another drug that cocaine users take to reduce the irritability experienced during heavy cocaine use. Some develop alcohol addiction in addition to their cocaine problem. An important metabolic interaction occurs when cocaine and alcohol are taken concurrently. Some cocaine is transesterified to cocaethylene, which is equipotent to cocaine in blocking dopamine reuptake (Hearn et al., 1991). Toxicity Other risks of cocaine use, beyond the potential for addiction, involve cardiac arrhythmias, myocardial ischemia, myocarditis, aortic dissection, cerebral vasoconstriction, and seizures. Death from trauma also is associated with cocaine use (Marzuk et al., 1995). Pregnant cocaine users may experience premature labor and abruptio placentae (Chasnoff et al., 1989). Attributing the developmental abnormalities reported in infants born to cocaine-using women simply to cocaine use is confounded by the infant's prematurity, multiple drug exposure, and overall poor pre- and postnatal care. Cocaine has been reported to produce a prolonged and intense orgasm if taken prior to intercourse, and its use is associated with compulsive and promiscuous sexual activity. Long-term cocaine use, however, usually results in reduced sexual drive; complaints of sexual problems are common among cocaine users presenting for treatment. Psychiatric disordersincluding anxiety, depression, and psychosisare common in cocaine users who request treatment. While some of these psychiatric disorders undoubtedly existed prior to the stimulant use, many develop during the course of the drug abuse (McLellan et al., 1979). Tolerance, Dependence, and Withdrawal Sensitization is a consistent finding in animal studies of cocaine and other stimulants. Sensitization is produced by intermittent use and typically is measured by behavioral hyperactivity. In human cocaine users, sensitization for the euphoric effect typically is not seen. On the contrary, most experienced users report requiring more cocaine over time to obtain euphoria, i.e., tolerance. In the laboratory, tachyphylaxis (rapid tolerance) has been observed with reduced effects when the same dose is given repeatedly in one session. Sensitization may involve conditioning (Figure 242). Cocaine users often report a strong response on seeing cocaine before it is administered, consisting of physiological arousal and increased drug craving (O'Brien et al., 1992). Sensitization in human beings has been linked to paranoid, psychotic manifestations of cocaine use based on the observation that cocaine-induced hallucinations are typically seen after long-term exposure (mean 35 months) in vulnerable users (Satel et al., 1991). Repeated administration may be required to sensitize the patient to experience paranoia. Since cocaine typically is used intermittently, even heavy users go through frequent periods of withdrawal or 'crash.' The symptoms of withdrawal seen in users admitted to the hospital are listed in Table 248. Careful studies of cocaine users during withdrawal show gradual diminution of these symptoms over 1 to 3 weeks (Weddington et al., 1990). Residual depression may be seen after cocaine withdrawal and should be treated with antidepressant agents if it persists (see Chapter 19: Drugs and the Treatment of Psychiatric Disorders: Depression and Anxiety Disorders). Pharmacological Interventions Since cocaine withdrawal generally is mild, treatment of withdrawal symptoms usually is not required. The major problem in treatment is not detoxification but helping the patient to resist the urge to restart compulsive cocaine use. Rehabilitation programs involving individual and group psychotherapy based on the principles of Alcoholics Anonymous and behavioral treatments based on reinforcing, cocaine-free urine tests result in significant improvement in the majority of cocaine users (Alterman et al., 1994; Higgins et al., 1994). Nonetheless, there is great interest in finding a medication that can aid in the rehabilitation of cocaine addicts. Numerous medications have been tried in clinical trials with cocaine addicts (O'Brien, 1997). While several drugs have been reported in individual studies to produce significant reductions in cocaine use, none has been found to be associated with consistent improvement in controlled clinical trials. The dopamine and serotonin systems have been the focus of many unsuccessful studies using both agonist and antagonist approaches. The concept that works well for opioid addiction, that of a long-acting agonist to satisfy drug craving and stabilize the patient so that normal function is possible, is difficult to transfer to the pharmacology of stimulants. Recent attention has been directed toward two novel approaches: a compound that competes with cocaine at the dopamine transporter and a vaccine that produces cocaine-binding antibodies. However, these should be regarded as innovative ideas that have yet to be shown to be clinically useful. For now, the treatment of choice for cocaine addiction remains behavioral, with medication indicated for specific coexisting disorders such as depression. Other CNS Stimulants Amphetamine and Related Agents Subjective effects similar to those of cocaine are produced by amphetamine,
dextroamphetamine, methamphetamine, phenmetrazine, methylphenidate and diethylpropion.
Amphetamines increase synaptic dopamine primarily by stimulating presynaptic
release rather than by blockade of reuptake, as is the case with cocaine.
Intravenous or smoked methamphetamine produces an abuse/dependence syndrome
similar to that of cocaine, although clinical deterioration may progress more
rapidly. Methamphetamine can be produced in small, clandestine laboratories
starting with ephedrine, a widely available nonprescription stimulant. It
became a major problem in the western Khat is a
plant material widely chewed in East Africa and Caffeine Caffeine, a mild stimulant, is the most widely used psychoactive drug in the world. It is present in soft drinks, coffee, tea, cocoa, chocolate, and numerous prescription and over-the-counter drugs. It increases norepinephrine secretion and enhances neural activity in numerous brain areas. Caffeine is absorbed from the digestive tract; it is rapidly distributed throughout all tissues and easily crosses the placental barrier (see Chapter 28: Drugs Used in the Treatment of Asthma). Many of caffeine's effects are believed to occur by means of competitive antagonism at adenosine receptors. Adenosine is a neuromodulator that influences a number of functions in the CNS (see Chapters 12: Neurotransmission and the Central Nervous System and 28: Drugs Used in the Treatment of Asthma). The mild sedating effects that occur when adenosine activates particular adenosine receptor subtypes can be antagonized by caffeine. Tolerance occurs rapidly to the stimulating effects of caffeine. Thus, a mild withdrawal syndrome has been produced in controlled studies by abrupt cessation of as little as one to two cups of coffee per day. Caffeine withdrawal consists of feelings of fatigue and sedation. With higher doses, headaches and nausea have been reported during withdrawal; vomiting is rare (Silverman et al., 1992). Although a withdrawal syndrome can be demonstrated, few caffeine users report loss of control of caffeine intake or significant difficulty in reducing or stopping caffeine if desired (Dews et al., 1999). Thus caffeine is not listed in the category of addicting stimulants (American Psychiatric Association, 1994). Cannabinoids (Marijuana) The cannabis plant has been cultivated for centuries both for the
production of hemp fiber and for its presumed medicinal and psychoactive
properties. The smoke from burning cannabis contains many chemicals,
including 61 different cannabinoids that have been identified. One of these, Surveys have shown that marijuana is the most commonly used nonlegal
drug in the A cannabinoid receptor has been identified in the brain (Devane et al., 1988) and cloned (Matsuda et al., 1990). An arachidonic acid derivative has been proposed as an endogenous ligand and named anandamide (Devane et al., 1992). While the physiological function of these receptors or their putative endogenous ligand has not been fully elucidated, they are widely dispersed, with high densities in the cerebral cortex, hippocampus, striatum, and cerebellum (Herkenham, 1993). Specific cannabinoid receptor antagonists have been developed, and these should facilitate understanding the role of this neurotransmitter system, not only in marijuana abuse but also in normal CNS functions. The pharmacological effects of Marijuana also produces complex behavioral changes, such as giddiness and increased hunger. Although some users have reported increased pleasure from sex and increased insight during a marijuana high, these claims have not been substantiated. Unpleasant reactions such as panic or hallucinations and even acute psychosis may occur; several surveys indicate that 50% to 60% of marijuana users have reported at least one anxiety experience. These reactions commonly are seen with higher doses and with oral rather than smoked marijuana, because smoking permits the regulation of dose according to the effects. While there is no convincing evidence that marijuana can produce a lasting schizophrenia-like syndrome, there are numerous clinical reports that marijuana use can precipitate a recurrence in people with a history of schizophrenia. One of the most controversial of the effects that have been claimed for marijuana is the production of an 'amotivational syndrome.' This syndrome is not an official diagnosis, but it has been used to describe young people who drop out of social activities and show little interest in school, work, or other goal-directed activity. When heavy marijuana use accompanies these symptoms, the drug often is cited as the cause, even though there are no data that demonstrate a causal relationship between marijuana smoking and these behavioral characteristics. There is no evidence that marijuana use damages brain cells or produces any permanent functional changes, although there are animal data indicating impairment of maze learning that persists for weeks after the last dose. These findings are consistent with clinical reports of gradual improvement in mental state after cessation of chronic high-dose marijuana use. Several medicinal benefits of marijuana have been described. These include antinausea effects that have been applied to the relief of side effects of anticancer chemotherapy, muscle-relaxing effects, anticonvulsant effects, and reduction of intraocular pressure for the treatment of glaucoma. These medical benefits come at the cost of the psychoactive effects that often impair normal activities. Thus, there is no clear advantage of marijuana over conventional treatments for any of these indications (Institute of Medicine, 1999). With the cloning of cannabinoid receptors and the discovery of an endogenous ligand, it is hoped that medications can be developed that will produce specific therapeutic effects without the undesirable properties of marijuana. Tolerance, Dependence, and Withdrawal Tolerance to most of the effects of marijuana can develop rapidly after only a few doses, but it also disappears rapidly. Tolerance to large doses has been found to persist in experimental animals for long periods after cessation of drug use. Withdrawal symptoms and signs are not typically seen in clinical populations. In fact, relatively few patients ever seek treatment for marijuana addiction. A withdrawal syndrome in human subjects has been described following close observation of marijuana users given regular oral doses of the agent on a research ward (Table 249). This syndrome, however, is seen clinically only in persons who use marijuana on a daily basis and then suddenly stop. Compulsive or regular marijuana users do not appear to be motivated by fear of withdrawal symptoms, although this has not been systematically studied. Pharmacological Interventions Marijuana abuse and addiction have no specific treatments. Heavy users may suffer from accompanying depression and thus may respond to antidepressant medication, but this should be decided on an individual basis considering the severity of the affective symptoms after the marijuana effects have dissipated. The residual drug effects may continue for several weeks. Psychedelic Agents Perceptual distortions that include hallucinations, illusions, and disorders of thinking such as paranoia can be produced by toxic doses of many drugs. These phenomena also may be seen during toxic withdrawal from sedatives such as alcohol. There are, however, certain drugs that have as their primary effect the production of perception, thought, or mood disturbances at low doses with minimal effects on memory and orientation. These are commonly called hallucinogenic drugs, but their use does not always result in frank hallucinations. In the late 1990s, the use of 'club drugs' at all-night dance parties became popular. Such drugs include methylenedioxymethamphetamine ('Ecstasy,' MDMA), lysergic acid diethylamide (LSD), phencyclidine (PCP), and ketamine. They often are used in association with illegal sedatives such as flunitrazepam (ROHYPNOL) or gamma hydroxybutyrate (GHB). The latter drug has the reputation of being particularly effective in preventing memory storage, so it has been implicated in 'date rapes.' The use of psychedelics received much public attention in the 1960s
and 1970s, but their use waned in the 1980s. In 1989, the use of
hallucinogenic drugs again began to increase in the While psychedelic effects can be produced by a variety of different drugs, major psychedelic compounds come from two main categories. The indoleamine hallucinogens include LSD, DMT (N,N-dimethyltryptamine), and psilocybin. The phenethylamines include mescaline, dimethoxymethylamphetamine (DOM), methylenedioxyamphetamine (MDA), and MDMA. Both groups have a relatively high affinity for serotonin 5-HT2 receptors (see Chapter 11: 5-Hydroxytryptamine (Serotonin): Receptor Agonists and Antagonists), but they differ in their affinity for other subtypes of 5-HT receptors. There is a good correlation between the relative affinity of these compounds for 5-HT2 receptors and their potency as hallucinogens in human beings (Rivier and Pilet, 1971; Titeler et al., 1988). The 5-HT2 receptor is further implicated in the mechanism of hallucinations by the observation that antagonists of that receptor, such as ritanserin, are effective in blocking the behavioral and electrophysiological effects of hallucinogenic drugs in animal models. However, LSD has been shown to interact with many receptor subtypes at nanomolar concentrations, and at present it is not possible to attribute the psychedelic effects to any single 5-HT receptor subtype (Peroutka, 1994). LSD LSD is the most potent hallucinogenic drug and produces significant
psychedelic effects with a total dose of as little as 25 to 50 The effects of hallucinogenic drugs are variable, even in the same
individual on different occasions. LSD is rapidly absorbed after oral
administration, with effects beginning at 40 to 60 minutes, peaking at 2 to 4
hours, and gradually returning to baseline over 6 to 8 hours. At doses of 100
Claims about the potential of psychedelic drugs for enhancing psychotherapy and for treating addictions and other mental disorders have not been supported by controlled treatment outcome studies. Consequently, there is no current indication for these drugs as medications. A 'bad trip' usually consists of severe anxiety, although at times it is marked by intense depression and suicidal thoughts. Visual disturbances usually are prominent. The bad trip from LSD may be difficult to distinguish from reactions to anticholinergic drugs and phencyclidine. There are no documented toxic fatalities from LSD use, but fatal accidents and suicides have occurred during or shortly after intoxication. Prolonged psychotic reactions lasting two days or more may occur after the ingestion of a hallucinogen. Schizophrenic episodes may be precipitated in susceptible individuals, and there is some evidence that chronic use of these drugs is associated with the development of persistent psychotic disorders (McLellan et al., 1979). Tolerance, Physical Dependence, and Withdrawal Frequent, repeated use of psychedelic drugs is unusual, and thus tolerance is not commonly seen. Tolerance does develop to the behavioral effects of LSD after three to four daily doses, but no withdrawal syndrome has been observed. Cross-tolerance among LSD, mescaline, and psilocybin has been demonstrated in animal models. Pharmacological Intervention Because of the unpredictability of psychedelic drug effects, any use carries some risk. Dependence and addiction do not occur, but users may require medical attention because of 'bad trips.' Severe agitation may require medication, and diazepam (20 mg orally) has been found to be effective. 'Talking down' by reassurance also has been shown to be effective and is the management of first choice. Neuroleptic medications (dopamine receptor antagonists; see Chapter 20: Drugs and the Treatment of Psychiatric Disorders: Psychosis and Mania) may intensify the experience. A particularly troubling aftereffect of the use of LSD and similar drugs is the occurrence of episodic visual disturbances in a small proportion of former users. These originally were called 'flashbacks' and resembled the experiences of prior LSD trips. There now is an official diagnostic category called the hallucinogen persisting perception disorder (HPPD) (American Psychiatric Association, 1994). The symptoms include false fleeting perceptions in the peripheral fields, flashes of color, geometric pseudohallucinations, and positive afterimages (Abraham and Aldridge, 1993). The visual disorder appears stable in half of the cases and represents an apparently permanent alteration of the visual system. Precipitants include stress, fatigue, entry into a dark environment, marijuana, neuroleptics, and anxiety states. MDMA ('Ecstasy') and MDA MDMA and MDA are phenylethylamines that have stimulant as well as psychedelic effects. MDMA became popular during the 1980s on college campuses because of testimonials that it enhances insight and self-knowledge. It was recommended by some psychotherapists as an aid to the process of therapy, although no controlled data exist to support this contention. Acute effects are dose-dependent and include tachycardia, dry mouth, jaw clenching, and muscle aches. At higher doses, the effects include visual hallucinations, agitation, hyperthermia, and panic attacks. MDA and MDMA produce degeneration of serotonergic nerve cells and axons in rats. While nerve degeneration has not been demonstrated in human beings, the cerebrospinal fluid of chronic MDMA users has been found to contain low levels of serotonin metabolites (Ricaurte et al., 2000). Thus there is possible neurotoxicity with no evidence that the claimed benefits of MDMA actually occur. Phencyclidine (PCP) PCP deserves special mention because of its widespread availability
and because its pharmacological effects are
different from those of the psychedelics such as LSD. PCP originally was
developed as an anesthetic in the 1950s and later was abandoned because of a
high frequency of postoperative delirium with hallucinations. It was classed
as a dissociative anesthetic because, in the anesthetized state, the patient
remains conscious with staring gaze, flat facies, and rigid muscles. PCP
became a drug of abuse in the 1970s, first in an oral form and then in a
smoked version enabling a better regulation of the dose. The effects of PCP
have been observed in normal volunteers under controlled conditions. As
little as 50 PCP binds with high affinity to sites located in the cortex and limbic structures, resulting in blocking of NMDA-type glutamate receptors (see Chapter 12: Neurotransmission and the Central Nervous System). LSD and other psychedelics do not bind NMDA receptors. There is evidence that NMDA receptors are involved in ischemic neuronal death caused by high levels of excitatory amino acids; as a result, there is interest in PCP analogs that block NMDA receptors but have fewer psychoactive effects. Tolerance, Dependence, and Withdrawal PCP is reinforcing in monkeys, as evidenced by self-administration patterns that produce continuous intoxication (Balster et al., 1973). Human beings tend to use PCP intermittently, but some surveys report daily use in 7% of users queried. There is evidence for tolerance to the behavioral effects of PCP in animals, but this has not been studied systematically in human beings. Signs of a PCP withdrawal syndrome were observed in monkeys after interruption of daily access to the drug. These include somnolence, tremor, seizures, diarrhea, piloerection, bruxism, and vocalizations. Pharmacological Intervention Overdose must be treated by life support, since there is no antagonist of PCP effects and no proven way to enhance excretion, although acidification of the urine has been proposed. PCP coma may last 7 to 10 days. The agitated or psychotic state produced by PCP can be treated with diazepam. Prolonged psychotic behavior requires neuroleptic medication such as haloperidol. Because of the anticholinergic activity of PCP, neuroleptics with significant anticholinergic effects, such as chlorpromazine, should be avoided. Inhalants Abused inhalants consist of many different categories of chemicals that are volatile at room temperature and produce abrupt changes in mental state when inhaled. Examples include toluene (from airplane glue), kerosene, gasoline, carbon tetrachloride, amyl nitrite, and nitrous oxide (see Chapter 68: Nonmetallic Environmental Toxicants: Air Pollutants, Solvents and Vapors, and Pesticides for a discussion of the toxicology of such agents). There are characteristic patterns of response for each substance. Solvents such as toluene typically are used by children. The material usually is placed in a plastic bag and the vapors inhaled. After several minutes of inhalation, dizziness and intoxication occur. Aerosol sprays containing fluorocarbon propellants are another source of solvent intoxication. Prolonged exposure or daily use may result in damage to several organ systems. Clinical problems include cardiac arrhythmias, bone marrow depression, cerebral degeneration, and damage to liver, kidney, and peripheral nerves. Death occasionally has been attributed to inhalant abuse, probably via the mechanism of cardiac arrhythmias, especially accompanying exercise or upper airway obstruction. Amyl nitrite produces dilation of smooth muscle and has been used in the past for the treatment of angina. It is a yellow, volatile, flammable liquid with a fruity odor. In recent years, amyl nitrite and butyl nitrite have been used to relax smooth muscle and enhance orgasm, particularly by male homosexuals. It is obtained in the form of room deodorizers and can produce a feeling of 'rush,' flushing, and dizziness. Adverse effects include palpitations, postural hypotension, and headache progressing to loss of consciousness. Anesthetic gases such as nitrous oxide or halothane are sometimes used as intoxicants by medical personnel. Nitrous oxide also is abused by food service employees, because it is supplied for use as a propellant in disposable aluminum minitanks for whipped-cream canisters. Nitrous oxide produces euphoria and analgesia and then loss of consciousness. Compulsive use and chronic toxicity rarely are reported, but there are obvious risks of overdose associated with the abuse of this anesthetic. Chronic use has been reported to cause peripheral neuropathy. |
Treatment of Drug Abuse and Addiction
|
The management of drug abuse and addiction must be individualized according to the drugs involved and to the associated psychosocial problems of the individual patient. Pharmacological interventions have been described for each category when medications are available. An understanding of the pharmacology of the drug or combination of drugs ingested by the patient is essential to rational and effective treatment. This may be a matter of urgency for the treatment of overdose or for the detoxification of a patient who is experiencing withdrawal symptoms. It must be recognized, however, that the treatment of the underlying addictive disorder requires months or years of rehabilitation. The behavior patterns encoded during thousands of prior drug ingestions do not disappear with detoxification from the drug, even after a typical 28-day inpatient rehabilitation program. Long periods of outpatient treatment are necessary. There probably will be periods of relapse and remission. While complete abstinence is the preferred goal, in reality most patients are at risk to slip back to drug-seeking behavior and require a period of retreatment. Maintenance medication can be effective in some circumstances, such as methadone for opioid dependence. The process can best be compared to the treatment of other chronic disorders such as diabetes, asthma, or hypertension. Long-term medication may be necessary, and cures are not likely. When viewed in the context of chronic disease, the available treatments for addiction are quite successful (McLellan et al., 1992; O'Brien, 1994). Long-term treatment is accompanied by improvements in physical status as well as in mental, social, and occupational function. Unfortunately, there is general pessimism in the medical community about the benefits of treatment, so that most of the therapeutic effort is directed at the complications of addiction, such as pulmonary, cardiac, and hepatic disorders. Prevention of these complications can be accomplished by addressing the underlying addictive disorder. For further discussion of alcoholism and drug dependency see Chapters
372 to 375 in Harrison's Principles of Internal Medicine, 16th ed., |
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 1719
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2024 . All rights reserved