| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Nissen Fundoplication
When persistent gastroesophageal reflux can not be effectively controlled by nonoperative treatment such as pills, potions, and dietary changes, a Nissen fundoplication offers remedial action and represents the first choice approach for the patient whose left upper quadrant and epigastrium have remained untouched by a surgical procedure and hence are free of adhesions. If there has been longstanding esophagitis and shortening of the esophagus, the simple wrap of a flap of gastric fundus around the esophagus may not be possible. In these patients, the Collis gastroplasty, lengthening the esophagus with a gastric tube of the lesser curvature in continuity, and a modified Nissen fundoplication of the remaining fundus and greater curvature dog ear will accomplish the same result as a single fundoplication (Figure III-21, A to G). Both operations can be performed by laparotomy and laparoscopy. In all patients, a preliminary esophagoscopy with four quadrant biopsies of the lower esophageal segment should have established the fact that there is no malignant transformation associated with longstanding esophagitis.
Nissen Fundoplication
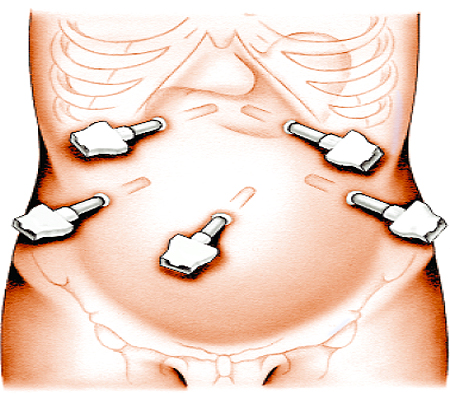
Step 1: Port sites
The approach is usually through five ports: the umbilical trocar for the placement of the laparoscope, two trocar sites on each side of the epigastrium close to the mid-costal margins, and two sites in the right and left mid-abdominal areas at the borders between upper and lower quadrants.
Nissen Fundoplication
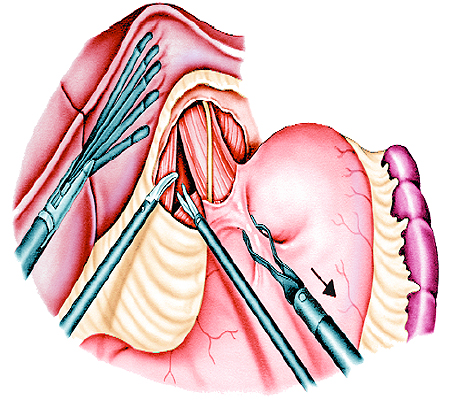
Step 2: 208. Exposure of the gastroesophageal junction
The left lobe of the liver is elevated with a sturdy fan retractor introduced through the right epigastric port. Although incision of the triangular ligament is occasionally required to facilitate this retraction, it is not undertaken on a routine basis because of occasional bothersome oozing of blood from that site. With gentle traction on the fundus of the stomach and on the esophagus, short gastric vessels along the upper reaches of the greater curvature and branches from the left gastric vessels along the lesser curvature are coagulated and divided to lend greater mobility to the GE junction. The areolar tissue around the hiatus is dissected and the phrenoesophageal ligament is incised, to expose the GE junction and the pillars of the diaphragmatic crus.
Nissen Fundoplication
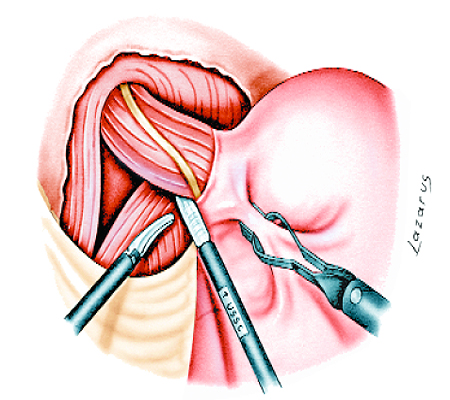
Step 3: Dissection and liberation of the abdominal esophagus
With continued traction to the left, on the anterior wall of the stomach below the GE junction, the abdominal esophageal segment is liberated in its entire circumference, starting from behind the junction upward into the mediastinum. The vagus nerves are identified and preserved during this dissection. By delineating the esophagus at its junction with the stomach, it is easier to keep the upward dissection close to the circumference of the esophageal tube and avoid injury to the left pleura by an errant scissors tip.
Nissen Fundoplication
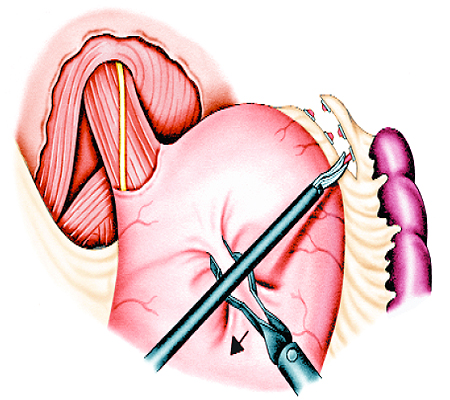
Step 4: Ligation and division of the short gastric vessels
In order to give full mobility to the fundus along the descending portion of the greater curvature, it may be necessary to divide three or four additional short gastric vessels, while taking great care to protect the spleen, which is usually pushed posteriorly by the pneumoperitoneum.
Nissen Fundoplication
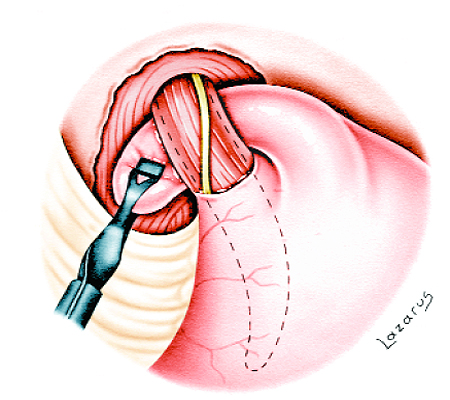
Step 5: Elevation of the gastric fundus
A Babcock clamp is passed behind the fully liberated esophagus, anterior to the left crural pillar. The wall of the fundus is elevated with a second Babcock clamp at a point on the fundus and apex of the greater curvature that is mobile and of sufficient length to pass behind the esophagus and wrap around its right side.
Nissen Fundoplication
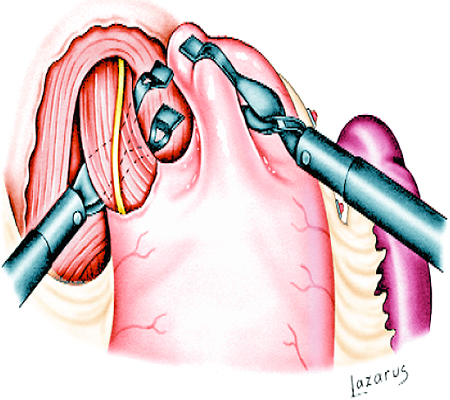
Step 6: Passage of the collar of fundus behind the esophagus
The future collar of fundus is grasped with the right-sided Babcock clamp and pulled behind the esophagus to the right anterior aspect of the GE junction. A large intraluminal bougie is advanced.
Nissen Fundoplication
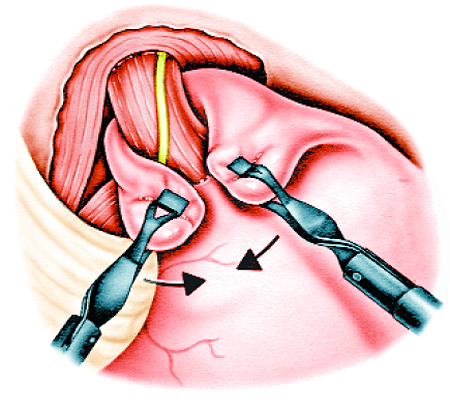
Step 7: Anterior approximation of the fundal wrap
The remaining left side of the fundus is elevated by a second Babcock clamp to meet with its right counterpart over the GE junction that is calibrated by the intraluminal bougie. This encounter serves in the appreciation of any number of parameters, for example, loose vs tight collar, unsatisfactory mobility of the wrap, insufficient height of the collar to ensure a safe placement of the sutures and to forecast a reliable functional result. All of these factors can be evaluated and corrected before the final step of closing the collar anteriorly.
Nissen Fundoplication
Step 8: Repair of the hiatus
With the right side of the collar held out of the way, on gentle traction to elevate the esophagus, the hiatus is repaired deep to the fundic flap with two to three sutures placed and tied with the previously mentioned intraluminal bougie in place.
Nissen Fundoplication
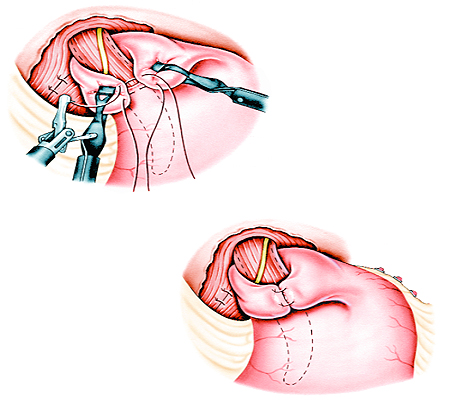
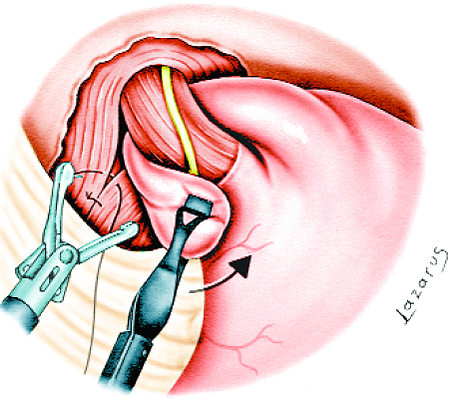
Step 9: Suture closure of the collar (Part I)
All that remains to be done is to close the collar anteriorly with two or three sutures. In order to prevent slippage of the collar into the mediastinum, the lower-most closing suture is taken through the anterior gastric wall, just below the GE junction.
Nissen Fundoplication
Step 10: Suture closure of the collar (Part 2)
A floppy wrap is obtained, with sutures tied over the bougie.
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 19080
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2025 . All rights reserved