| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
VASCULAR ACCESS Early Diagnosis and Treatment of Complications
Co-director of Nephrology and Transplantation and the
Medical Director of the Clinical Laboratory, Austin Diagnostic Clinic,
Today we are spending about a billion dollars each year for vascular access, and about 25 percent of all of our hospital admissions for dialysis patients are for dialysis access problems. What we clearly need is a more effective and a better planned strategy for the management of vascular access.
Primary components of a vascular access strategy
This represents what I think are the primary components of that strategy. Let me say that about 75 percent of my talk is going to be taken from the DOQI Guidelines, about 25 percent of it is from my own experience, and I'm making up about 5 percent of it. We need to maximize arterial venous fistula use, decrease incidence of thrombosis, and develop quality assurance programs that detect access at risk, tract complications, implement procedures to increase access longevity.
Types of vascular access
We have three types of vascular access from which to choose: The AV fistula, the prosthetic bridge graft, and the tunneled cuffed catheter, not all of which are cuffed actually.
AV fistula -- advantages
The AV fistula, as you know, has certain advantages, and it actually has advantages at all ages. It is 67 percent better at age 40. It is still 24 percent better at age 65 in comparison to a graft. The infection rate is one tenth that seen in the graft.

AV fistula - disadvantages
It does have some certain disadvantages. Some patients have an unacceptable anatomy; there is a slow maturation, in some patients these accesses never mature; it is somewhat more difficult to cannulate than a graft, as many of you are aware; and there are some cosmetic disadvantages because it tends to increase in size with age.
AV fistula: placement preferences
According to the DOQI Guidelines, these are the order of preference for AV fistula placement. First choice is the radiocephalic, which is at the wrist. The second choice is the brachiocephalic, an upper arm AV fistula. The third choice, which when we created the DOQI Guidelines we felt was basically equivalent to a prosthetic bridge graft is the brachiobasilic transposition.
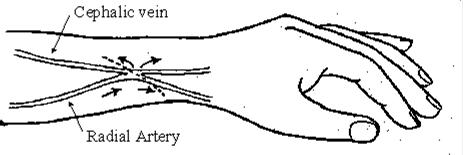
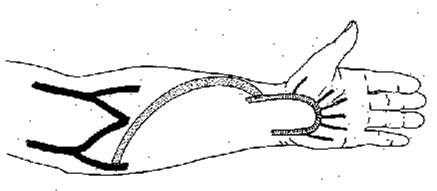
Radiocephalic fistula
The radiocephalic fistula can be created with a side-to-side anastomosis or end-to-side anastomosis at the wrist.
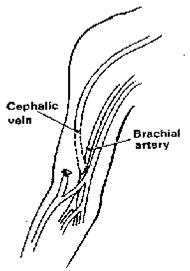
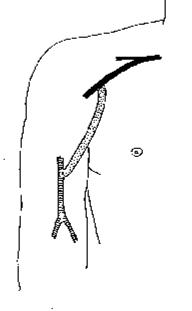
Brachiocephalic fistula
The brachiocephalic involves anastomosis of the cephalic vein to the brachial artery at the elbow, creating an upper arm fistula in the lateral aspect of the arm.
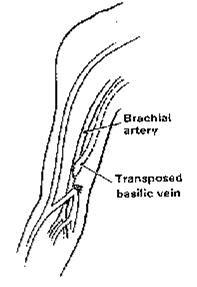
Brachiobasilic transposition fistula
The brachiobasilic transposition involves the basilic vein, which has to be freed up and transposed laterally in order for it to be accessible for cannulation.
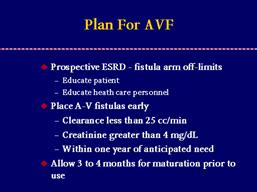
Importance of early planning for AV fistula insertion
It is important that we plan for AV fistulas early. This has been touched on already. When we see prospective end-stage renal disease patients, we need to put their fistula arm off limits and educate the patient to that fact and educate health care personnel as well. AV fistula needs to be created early. When the clearance gets less than 25 ccs per minute, that's creatinine clearance, a serum creatinine of greater than 4 ml/dl in general, although that's variable, but within one year of anticipated need. And we need to allow three to four months of maturation prior to usage.
Secondary AV fistula creation opportunities
We also need to keep in mind that the patient needs to be evaluated for an AV fistula after every access failure because the presence of a prosthetic bridge graft in the lower arm will cause veins in the upper arm to dilate to the point that they can become ideal candidates for the creation of what we refer to as a secondary AV fistula.
AV fistula complications
There are certain complications that occur with fistulas: Ischemia, venous stenosis, thrombosis, aneurysm formation, and infection. I would like to touch on each of those just for a moment.
AV fistula complications: ischemia
Ischemia has already been covered. It involves hands and fingers. It can have dire consequences, as you saw in the slides that were presented. Actually with fistulas, it is not very prominent. That is because it is generally preventable through physical examination prior to creation. But when it is present, immediate treatment is mandatory.
AV fistula complications: venous stenosis
Venous stenosis in the fistula is not anywhere near as common as with the prosthetic bridge graft. But when it does occur, it is a more serious problem than with the prosthetic bridge graft. The most common site for it to occur is adjacent to the arterial anastomosis. Screening tests such as venous pressure and flow measurements are poor screening tests for this problem. Recirculation, which is a poor test for prosthetic bridge grafts turns out to be a relatively good screening test for this problem. Treatment success is not as good as with the prosthetic bridge graft, but we do need to keep in mind that the fistula will keep open with very low flows, much lower than a graft. A graft will frequently clot if it gets below about 800, certainly below 600. A fistula can stay open with 200 blood flow.
AV fistula complications: thrombosis
Thrombosis also is not as common as with a graft, it is about one- sixth as common. When it does occur, it denotes a more serious problem. When it occurs early, it is generally secondary to poor inflow. When it occurs late, it is generally secondary to venous stenosis, and salvage is not particularly good with either percutaneous treatment or surgical treatment.
AV fistula complications: aneurysm formation
Aneurysm formation occurs in these, as we all know. With passage of time, blood flow increases and the fistula dilates. But still the most common cause of aneurysm is the problem of one-site-itis, continuing to cannulate the same site. It needs to be repaired if there is thinning of the skin, alteration of the skin, spontaneous bleeding, or if it limits potential needle cannulation sites, or if it is creating a cosmetic problem for the patient.
Prosthetic bridge graft
Prosthetic bridge grafts have certain advantages: Wide applicability-- you can put one in almost anyone; you can use them quite early, within the first two to three weeks; they work well initially; and they present a large cannulation area. They have disadvantages, the primary one which is venous stenosis, which leads to inadequate dialysis; recurrent thrombosis; it causes the prosthetic bridge graft to have a limited life expectancy; and then we also have the problem of infection.
Planning ahead for an AV graft placement
It is important when we have a patient who is going to start dialysis that we plan for the placement of the prosthetic bridge graft as well. Just putting their arm off limits holds here as it does for the fistula. But it is important that we not place the prosthetic bridge graft too early. It doesn't need to be placed more than three to six weeks before it is needed. We need to allow two to three weeks' maturation prior to usage.
Common AV graft configurations: straight graft
There are several configurations, some of which you've already seen. The straight graft in the lower arm, which has the lowest flow of all the choices;
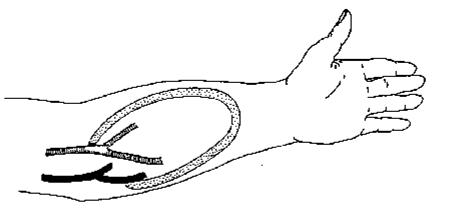
Common AV graft configurations: loop graft
the loop graft in the lower arm, which has a higher flow, generally in the range of about 1,200 cc/minute;
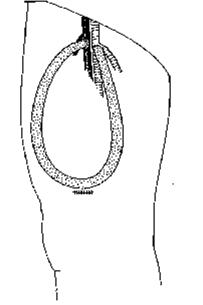
Common AV graft configurations: upper arm graft
the upper arm graft, which has even higher flow;
Common AV graft configurations: thigh graft
and then the thigh graft which, I agree, is an excellent choice for many patients. We see very few problems with these, of course, in the thigh graft. Then there are some novel applications that are sometimes used.
Prosthetic AV graft complications
The complications that occur with the prosthetic bridge graft consist of venous stenosis, thrombosis, infection, pseudo aneurysm formation, and ischemia.
Prosthetic AV graft complications: venous stenosis
Venous stenosis is the most common problem, and it results in inefficient dialysis, which is worse when you try to use high blood flow. It leads to thrombosis; missed and delayed treatments, which contribute to morbidity and mortality of patients; and also this has an adverse economic effect on the dialysis facility.
PBG graft venous stenosis: prospective diagnosis and treatment
It is important that we screen for venous stenosis. It is important that all dialysis facilities establish a prospective program for screening venous stenosis and treating patients prospectively.
Screening for venous stenosis
The techniques, and I'm not going to go into detail on these,
but the primary techniques--dynamic venous pressure measurements; static venous
pressure measurements; intra-access flow, which is the best of the choices;
supplemental techniques, such as physical examination, which is an excellent
technique. Many nephrologists do not like to put their hands on a patient, but
if they do, they find they can get a lot of information. But it's something to
consider. Clinical parameters are important, such as swelling of the arm, the
slide you saw earlier, frequent clotting, things of that sort. Recirculation is
an extremely poor test, probably not worth doing. Unexplained decreases in Kt/v
and
Treatment of venous stensosis
When you treat the patient, you have two choices: Surgical, percutaneous transluminal venous angioplasty. The choice of this technique should depend upon the local expertise that is available. The important thing is that abnormal parameters these are physiological, hemodynamic, clinical parameters that must return to normal post-treatment. If they do not, the patient receives sham treatment.
Prosthetic AV graft complications: thrombosis
Thrombosis--national rates about 1 per patient per year. Eighty-five to 90 percent of these are associated with venous stenosis. Eighty percent of graft loss is associated with uncorrectable loss of patency associated with thrombosis.
Treatment of AV graft thrombosis
When you treat patients with thrombosis, you again have two choices: Surgical and thrombolysis, which can be done in several different ways. The choice depends upon local expertise, should depend on local expertise.
Essential elements of treatment
The essential elements of treatment are extremely important. This should be done in a timely fashion. Central venous catheters must be avoided. There is no excuse for using a central venous catheter in a patient who has a thrombosed graft. Angiography is mandatory. These patients have venous stenosis-- it has to be diagnosed; it has to be corrected. This is an outpatient treatment. There is no excuse for admitting the patient to the hospital for these treatments. Abnormal parameters need to return to normal. The parameters that suggest venous stenosis in every case should be evaluated for the creation of a secondary AV fistula. To do less than this is to offer the patient less than optimum therapy.
Prosthetic AV graft complications: infection
Infection is a very serious complication. Frequency is about 1.3 episodes for every 100 dialysis months. Staph aureus is the most organism. As has already been pointed out, this needs to be treated aggressively with antibiotics, also surgical therapy, either local resection or removal of the graft.
Prosthetic AV graft complications: pseudoaneurysm formation
Pseudoaneurysm formation is another problem. The most common cause, again, one-site-itis. These need to be treated when the pseudoaneurysm exceeds twice the diameter of the graft or is rapidly increasing in size, there is thinning of the skin overlying the pseudo aneurysm, alteration of the skin, spontaneous bleeding, or when it limits potential cannulation sites to the degree that you're having difficulty dialyzing the patient.
Prosthetic AV graft complications: ischemia
Ischemia is a more frequent problem with grafts than it is with fistulas. As has been pointed out quite well, I think, it is because the access offers low-resistance bypass to the hand or to the foot according to where the access is created. It takes two forms. Primary ischemia is just inadequate blood flow, and then the steal phenomenon which has been pointed out. It is generally seen early. Not always, but generally. Immediate treatment is mandatory to prevent loss of digits and limbs.
Tunneled cuffed catheter access
That brings us then to the third type of access, which is the tunneled cuff catheter. These catheters are beginning to be used in more situations as temporary access, as a back-up access for a failed access, even CAPD, as a bridge access to allow maturation of peripheral accesses, and as a permanent access.
Tunneled cuffed catheter: advantages and disadvantages
It has the advantages of wide applicability, it is easily placed, can be used immediately. But it has the disadvantages of poor flow, there are none of them that give good flow; loss of function; and the problem of infection. We are seeing better flow with newer catheters that are coming on the market, however. There is a very important relationship between size and flow, which is intuitive.
Importance of catheter size
Diameter is very important. Resistance decreases proportionate to the diameter raised to the 4th power. For that reason, a 19 percent increase in diameter will increase flow two-fold. Catheter length is less important. A 19 percent increase in diameter will compensate for doubling of length because resistance is directly proportionate to length not raised to any power.
Prepump pressure monitoring
Prepump pressure monitoring is extremely important when you are using catheters because they are high-resistance systems. The prepump pressures are likely to be lower when catheters are used. This causes a partial collapse of the pump segment of the tubing. That causes the flow meter to be grossly inaccurate, more than it normally is. It is normally grossly inaccurate, and this causes it to be even more so. So prepump pressure should not be allowed to fall below -200 mm of mercury.
Catheter placement
Catheter placement is extremely important. The right internal jugular is the first choice. There is no second choice, unfortunately. Sometimes you have to put them some place else, but there is no good second site, unfortunately. The internal jugular has the lowest risk of central venous stenosis and also the lowest risk of puncture-related complications, especially with ultrasound guidance, which I think should be considered mandatory. If you use ultrasound guidance for the placement of these catheters, you reduce your complication rate to zero.
Catheter insertion technique
Catheter insertion needs to be done, as I say, with real-time ultrasound guidance. Fluoroscopy is mandatory because tip placement is extremely important. The tip needs to be placed well within the atrium, not at the junction between the superior vena cava and the atrium, but well within the atrium.
Tunneled cuffed catheter complications: poor flow
Flow problems occur early and are due to poor placement in most instances. These are generally preventable at the time of placement. Late flow problems are related to thrombosis, and unfortunately thrombosis is a way of life with catheters. It's a very common problem.
Tunneled cuffed catheter complications: catheter thrombosis
There are a number of factors that lead to thrombosis, most of which are not well defined.
Types of catheter thrombosis
You can divide thrombi into intrinsic and extrinsic categories.
Extrinsic thrombosis
The extrinsic categories are mural thrombus, which is a thrombus attached to the vessel wall; the atrial thrombus, which presents as a mass within the atrium--neither one of these are very common; the central venous thrombus, which is more common.
Extrinsic thrombosis: central vein thrombosis
Its exact incidence is really not clear because we only recognize it when it becomes symptomatic. Many of them are not symptomatic. When they are recognized, the treatment is to remove the catheter and anticoagulate the patient for a period of probably three months.
Catheter thrombosis: intrinsic thrombosis
Of the intrinsic thrombi there are three types: Intraluminal, which is within the lumen of the catheter; catheter tip thrombus, which is at the tip of the catheter--and both of these are related to the same problem--inadequate heparin filling the catheter should be over filled with heparin; loss of heparin from the catheter for some reason; or inadequate flushing of blood from the catheter. They actually don't occur very commonly.
Fibrin sheath
The fibrin sheath is the one that occurs most commonly, and this is what it looks like. This catheter is in the process of being removed. The catheter has been pulled back. It used to extend down to here. What you see from that arrow down is the fibrin sheath, like a windsock flapping in the breeze, so to speak. It starts at the venotomy site and extends the full length of the catheter.
Fibrin sheath formation
Fibrin sheath formation is very common. It probably occurs in 100 percent of catheters, but it doesn't always cause problems. It is a sleeve of fibrin that encases the catheter and creates a flap valve at the tip. Can it be prevented? It's not really clear. Perhaps not. There is some suggestion that perhaps systemic anticoagulation may help.
Treatment of catheter thrombosis
Treatment of thrombus, primary, is treated within the dialysis facility. It consists of urokinase intraluminal, which can be quite effective. It can also be treated mechanically. Secondary treatment is treatment outside of the dialysis facility, which consists of three things, one of which you can't see: Fibrin sheath stripping, catheter exchange over a guidewire. Fibrin sheath stripping is insertion of a (nitenol) loop through the femoral vein, going up, snaring the catheter, stripping it to get rid of the sheath, which is then embolized. Catheter exchange over a guidewire--just remove the catheter, put a new one in. But you have to be careful you don't put the new one back into the old fibrin sheath that may still be there. And then the last here is urokinase infusion, which has been used but is not as effective as these other two.
Tunneled cuffed catheter complications: infection
Infection, three types: Exit-site infection, tunnel infection, and catheter-related bacteremia.

Exit-site infection
Exit-site infection is defined as localized reaction with no systemic symptoms and negative blood cultures. It is treated locally. You need to change the catheter if there is worsening of the local signs or failure to respond to treatment and the patient needs to be monitored for change of category. In other words, if the patient starts having chills and fever and has a positive blood culture, it is no longer an exit-site infection.

Tunnel infection
The tunnel infection is defined as infection above the cuff. You can have infection below the cuff with an exit-site, but this is above the cuff with negative blood cultures. That does not occur very often. The reason why is these catheters move back and forth within the tunnel. If you get a tunnel infection, you're going to have bacteremia very quickly. So you can see this with bacteremia and generally do not see it by itself. The treatment is parenteral antibiotics and get rid of the catheter.
Catheter-related bacteremia
Catheter-related bacteremia is a very frequent complication, unfortunately. It is generally Staph. Secondary complications are very serious, all the way up to death in the current 20 to 30 percent of the cases. So it is a serious problem. There are two issues that we have to address when we have catheter-related bacteremia. One is what to do about the infection, and the other is what to do about the catheter.
Catheter-related bacteremia: definition and categorization
The definition here of catheter-related bacteremia is a positive blood culture with no other obvious cause. Now it doesn't really matter if there is another obvious cause. If the blood culture is positive, you still have to do something about the catheter because of the problem of biofilms. These infections fall into three categories: Minimum symptoms with a normal exit site, which is perhaps the most common that we see; minimum symptoms with an abnormal exit site; and severe symptoms of septicemia.
Catheter related bacteremia: minimal symptoms, normal exit site
The first is defined as a positive blood culture with almost no symptoms, maybe just fever and that's it, and a normal exit site. The treatment that we use is start them on antibiotics immediately and exchange the catheter over a guidewire within 24 to 48 hours and continue antibiotic treatment for three weeks. That is heresy to the infectious disease specialists, but we have to dialyze these patients. When we do this, we find that we have an 85 percent cure rate. To be a cure rate, they have to be clear of infection for nine weeks, by our definition.
Catheter related bacteremia: minimal symptoms, abnormal exit site
The second category is the patient with positive blood cultures, minimum symptoms, but with an abnormal exit site. The exit site is infected. These patients we start on antibiotics immediately, exchange the catheter over a guidewire 24 to 48 hours later, but do so by creating a new tunnel and a new exit site, retaining the old venotomy site, which is important. If you lose the venotomy site, you may never be able to put a catheter in that site again. And as I said, there are no good second choices as far as site is concerned. And then continue antibiotic treatment.

Catheter related bacteremia: severe symptoms
The third is severe symptoms, which is positive blood cultures with symptoms of septicemia. In these patients we have no choice. Treat them with antibiotics, pull the catheter and leave it out until they are clear, and then try to replace it wherever you can.
Concluding remarks
In summary, vascular access is a very important part of the management of the dialysis patient. As professionals caring for the end-stage renal disease patient, you have to become involved. You have to be part of the team managing these and help to devise strategies to maximize arterial venous fistula use, thereby minimizing prosthetic bridge graft usage, decrease the incidence of thrombosis through prospective screening and treatment programs, and develop quality assurance programs to increase your access longevity. Thank you very much.
References
1. NKF-DOQI clinical practice guidelines for vascular access. National Kidney Foundation-Dialysis Outcomes Quality Initiative. Am J Kidney Dis 1997 Oct (4 Suppl 3):S150-S191.
2. NKF-DOQI guidelines on the internet.
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 7737
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2025 . All rights reserved