| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Coronary Artery Disease
Coronary Atherosclerosis
The most common heart disorder in the
Although there is disagreement among authorities with regard to the origin of lesions, there is agreement that atherosclerosis is a progressive disease and that its progress can be curtailed and in some cases reversed.
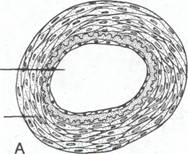
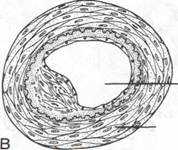
Pathophysiology. The functional lesion of atherosclerosis is called the atheroma. Atherosclerosis begins when the waxy cholesterol atheroma, which looks like pearly gray mounds of tissue, becomes deposited on the intima of the major arteries. These deposits interfere with the absorption of nutrients by the endothelial cells that compose the vessel lining and obstruct blood flow by protruding into the lumen of the vessel (fig.1). The vascular endothelium in involved areas becomes necrotic and then scarred, further compromising the lumen and impeding the flow of blood.
Cardiovascular, Circulatory, and Hematologic Function
|
|
|
|
|
Partially obstructed lumen with atheroma |
|
Lumen Smooth muscle layer |
|
Smooth muscle |
Figure 1. Cross-section of a normal and an atherosclerotic artery. (A) Cross-section of normal artery showing patent lumen. (B) Cross-section of artery showing atheroma and diminished patency of artery lume
At sites such as these where the lumen is narrowed and the wall rough, there is a great tendency for clots to form, which explains why intravascular coagulation, followed by thromboembolic disease, is among the most important complications of atherosclerosis.
|
|
|
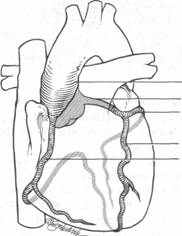
Aorta Left coronary artery Left circumflex artery Left anterior descending artery Right coronary artery |
Other clinical manifestations of coronary artery disease may be ECG changes, ventricular aneurysms, dysrhythmias, and sudden death.
the inhalation of smoke increases the blood carbon monoxide level. Hemoglobin, the oxygen carrying component of blood, combines more readily with CO then with O2. Thus, the oxygen being supplied to the heart is severely limited, which makes the heart work harder to produce the same amount of energy
nicotinic acid in tabacco products triggers the release of catecholamines, which cause arterial constriction. Blood flow and subsequent oxygenation are compromised.
cigarette smoking increases platelet adhesion, leading to higher probability of thrombus formation.
B. Elevated Blood Pressure is the most insidious of all risk factory because it is asymptomatic until hypertension is well advanced. An elevated blood pressure creates a very high pressure gradient against which the left ventricle must pump. The continued high pressure forces the myocardial oxygen demands to exceed the supply. The initiates the vicious cycle of pain associated with coronary artery disease.
Early detection of high blood pressure and compliance with a therapeutic regimen can prevent the serious consequences associated with untreated elevated blood pressure.
C. Hyperlipidemia . The association of elevated blood lipids with coronary artery disease has been established through epidemiologic studies. Lipids are mixed group biochemical substances that may be manufactured by the body or derived from metabolism of ingested substances. An endogenous lipid is one produced by the normal metabolic functions of the body; an example of an endogenous lipid is sterol. An exogenous lipid is one derived from a source external to the body, such as a food that is high in fat.
Lipids have the common property of being more soluble in fat or organic solvents than in water. In the blood, the principal lipids are cholesterol and triglycerides; an elevation of one or both is referred to as hyperlipidemia. To render them suitable for transport in the blood, the lipids are attached to a variety of proteins the resulting product is called a lipoprotein. The presence of lipoproteins in the blood is lipoproteinemia.
The lipoproteins are described clinically by their respective densities. Each lipoprotein has a distinct function in the metabolism of exogenous and endogenous lipids. Some, such as LDL (low-density lipoprotein), are belleved to play a role in the aggressiveness of the development of coronary heart disease. An excessive amount of lipoproteins in the blood is called hyperlipoproteinemia
Composition, Sources, and Functions of Lipoproteins Present in Plasma
Lipoprotein |
Composition |
Source |
Function |
Linked to coronary Heart Disease |
|
High density lipoproteins (HDL); Low density lipoproteins (LDL); - Intermediate low density (ILDL); - Very low density lipoproteins (VLDL) - Chylomicrons |
- Proteins 35% 60%- Phospholipid34% - 44% - Cholesterol 20%- 28% - Protein 20% - 25% - Phospholipid 25% - Triglyceride 14% - Cholesterol 46% Intermediary between LDL and VLDL Protein 10% -Phospholipid 20% -Cholesterol 5% -Triglyceride 65% -Protein 2% - Phospholipid 6% - 9% -Cholesterol 2% - Triglyceride 85% - 95% Liver From breakdown of VLDL Endogenous High dietary intake of CHO Dietary fat, exogenous |
Lowers LDL Transport cholesterol from liver to periphery Intermediate in transformation of VLDL to LDL Transports triglycerides from liver to periphery and serves as precursor to LDL Removes cholesterol from liver |
No Yes Yes Yes No |
|
There are five types of hyperlipidemia. The next table describes the five types the lipoprotein abnormality, and the potential clinical outcomes of elevated levels. Determining the underlying lipid abnormality by blood studies is essential before suggesting dietary control
Risk Factors for Atherosclerosis
|
Nonmodifiable Risk Factors |
Modifiable Risk Factors |
|
Positive family history; Increasing age; Sex Occurs three times more often in women; Race Higher incidence in blacks than in whites; Geography Higher incidence in industrialized regions |
Hyperlipidemia; Elevated blood pressure Cigarette smoking Elevated blood glucose (diabetes mellitus) Obesity Physical inactivity Stress Use of oral contraceptives Personality traits such as highly competitive, aggressive, or ambitious |
Hyperlipidemia may be primary or secondary. Primary hyperlipidemia is generally a hereditary disorder and is the rarest of phenotypes. The secondary type occurs as manifestation of numerous other diseases, including hypothyroidism, nephritic syndrome, diabetes mellitus and alcoholism. Therapy consists of treating the basic disorder.
Primary Hyperlipidemias and Associated Clinical Features
|
Phenotype |
Dominant Lipids |
Dominant Lipoproteins |
Clinical Features of elevated levels |
|
I (rare) II (common) A B III (uncommon) IV (uncommon) V (uncommon) |
Triglycerides Cholesterol Cholesterol Triglycerides Cholesterol Triglycerides Triglycerides Triglycerides |
Chylomicron LDL LDL ILDL VLDL Chylomocron VLDL |
Xanthoma Enlarged liver Pancreatitis Premature atherosclerosis Xanthoma Premature atherosclerosis Xanthoma Glucose intolerance Hyperuricemia Premature atherosclerosis Xanthoma Enlarged liver Pancreatitis Glucose intolerance Hyperuricemia Premature atherosclerosis |
For some individuals, the control of
fat consumption is an important factor in preventive nutrition. Dietary fat may
be regulated by changing the total amount or the type of fat in the diet, or
both. Assisting the patient to modify dietary fat intake through effective
counseling requires an understanding to the differences between saturated and
polyunsaturated fatty acids, cholesterol, medium-chain triglycerides, and
various other fractions, as well as of their functions in the human body.
No single diet or drug will be effective in all conditions in lowering the particular elevated lipid abnormality, but in most people with such an abnormality the level can be brought within the upper normal range.
For patients in whom diet alone cannot normalize the specific lipid, there are several medications that have a synergistic effect when taken with prescribed diet. These agents are shown to be biochemically effective, in that elevated lipoprotein concentration tends to return toward normal, and manifestations of the abnormalities, such as xanthomas (yellow papules in the skin caused by lipid deposits), may disappear. Drug treatment also varies with the type of hyperlipidemia. The drugs used are usually grouped into two type those that decrease lipoprotein synthesis such as nicotinic acid and clofibrate, and those that increase lipoprotein breakdown (catabolism), such as cholestyramine, sitosterol and D-thyroxine.
Harmful side effects can occur from the use of these drugs. Drug therapy is, therefore, reserved for the high-risk patient and is not regarded as a viable substitute for dietary modification. The usefulness of drugs in reversing coronary heart disease is still under investigation. It is however, broadly accepted that preventive nutrition can have a significant impact on coronary heart disease.
Hyperglycemia. The relationship of elevated blood glucose and increased evidence of coronary heart disease is substantiated. Hyperglycemia fosters increased platelet aggregation, wich can lead to thrombus formation. A high level of glucose (as is seen in some cases of adult onset diabetes) is said to cause damage to cells of the smooth muscle lining the vessels. The damaged vessel walls foster the growth of atheromas.
Other risk factors such as obesity and hypertension must be brought under control in addition to hyperglycemia. Control of hyperglycemia without modification of other risk factors does not reduce the risk of coronary heart disease.
Behavior Patterns of Coronary Prone Persons. It is believed that stress and certain behaviors contribute to the pathogenesis of coronary ( atheroscleratic) heart disease.
Psychobiologic and epidemiologic studies have investigated behaviors that characterize people who are prone to coronary artery disease: competitive striving for achievement exaggerated sense of time urgency, aggressiveness and hostility. A person who manifests these behaviors is classified as type. A coronary prone. It appears that, in addition to reducing other risk factory (smoking, dietary fats), such a person should take steps to alter life style and long-term habits.
The type A behavior pattern has been widely accepted as a risk factor for coronary heart disease. Contemporary research indicates that it may not be as significant as was once thought but there is not yet conclusive evidence of its precise role.
1.3. Gerontologic Consideration
Atherosclerotic coronary artery disease is not a function of aging. Aging does, however, produce changes in the integrity of the lining of the walls of arteries (arteriosclerosis), thus impeding blood flow and tissue nutrition. These changes are often sufficient to diminish oxygenation and increase myocardial oxygen consumption (MVO2). The result can be debilitating angina pectoris and eventually congestive heart failure.
Coronary heart disease is often preceded or accompanied by conditions that may incresa one s likelihood of morbidity. These conditions are referred to as risk factors. They are considered nonmodifiable if they are beyond personal control, such as age. If they are amenable to personal control, such as smoking, they are considered to be modifiable. Risk factor identification and modification are major thrusts of coronary heart disease prevention and treatment.
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 1221
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2025 . All rights reserved