| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
History and Principles of Anesthesiology
Overview
|
Prior to 1846, attempts to provide comfort during operative procedures were minimally effective and the development of surgery was necessarily limited. William T.G. Morton's public demonstration of ether in that year revolutionized medical care throughout the world. The evolution of anesthesiology as a medical specialty has facilitated the success of modern, complex surgical procedures. Beyond the obtundation of consciousness and creation of a quiescent surgical field, anesthesiology applies principles of physiology, pathophysiology, and pharmacology to assess and reduce surgical risk, maintain homeostasis, attenuate the surgical stress response, and provide analgesia. In this chapter, we explore the salient features of the preoperative, intraoperative, and postoperative periods, highlighting recent discoveries including anesthetic receptor specificity, identification of the neural correlates of consciousness, and new technology to assess levels of awareness. |
History of Surgical Anesthesia
|
Anesthesia before 1846 Surgical procedures were uncommon before 1846. Understanding of the pathophysiology of disease and of the rationale for its treatment by surgery was rudimentary. Aseptic technique and the prevention of wound infection were almost unknown. In addition, the lack of satisfactory anesthesia was a major deterrent. Because of all these factors, few operations were attempted, and mortality was frequent. Typically, surgery was of an emergency naturefor example, amputation of a limb for open fracture or drainage of an abscess. Fine dissection and careful technique were not possible in patients for whom relief of pain was inadequate. Some means of attempting to relieve surgical pain were available and, in fact, had been used since ancient times. Drugs like alcohol, hashish, and opium derivatives, taken by mouth, provided some consolation. Physical methods for the production of analgesia, such as packing a limb in ice or making it ischemic with a tourniquet, occasionally were used. Unconsciousness induced by a blow to the head or by strangulation did provide relief from pain, although at a high cost. However, the most common method used to achieve a relatively quiet surgical field was simple restraint of the patient by force. It is no wonder that surgery was looked upon as a last resort. Although the analgesic properties of both nitrous oxide and diethyl ether had been known to a few for years, the agents were not used for medical purposes. Nitrous oxide was synthesized by Priestley in 1776, and both he and Humphry Davy some 20 years later commented upon its anesthetic properties (Faulconer and Keys, 1965). Davy in fact suggested that '. . . it may probably be used with advantage during surgical operations in which no great effusion of blood takes place.' Another 20 years passed before Michael Faraday wrote that the inhalation of diethyl ether produced effects similar to those of nitrous oxide. However, except for their inhalation in carnival exhibitions or to produce 'highs' at 'ether frolics,' these drugs were not used in human beings until the midnineteenth century. Greene (1971) has presented an analysis of the reasons for the introduction
of anesthesia in the 1840s. The time was then right, since concern for the
well-being of one's fellows, a humanitarian attitude, was more prevalent than
it had been in the previous century. 'So long as witches were being
burned in Public Demonstration of Ether Anesthesia Dentists were instrumental in the introduction of both diethyl ether
and nitrous oxide. They, even more than physicians, came into daily contact
with persons complaining of pain; often, as a by-product of their work, they
produced pain. It was at a stage show that Horace Wells, a dentist, noted
that one of the participants, while under the influence of nitrous oxide,
injured himself yet felt no pain. The next day Wells, while breathing nitrous
oxide, had one of his own teeth extracted, painlessly, by a colleague.
Shortly thereafter, in 1845, Wells attempted to demonstrate his discovery at
the William T. G. Morton, a The story of this classical demonstration in 1846 has been retold
countless times. The operating room ('ether dome') at the Following initial disbelief, news of the successful demonstration
spread rapidly. Within a month, ether was in use in other cities of the The lives of those involved in the introduction of surgical anesthesia did not have so salubrious an outcome. Morton initially tried to patent the use of ether to produce anesthesia and, when this failed, patented instead his device for its administration. Considerable wrangling ensued as to who was the legitimate discoverer of anesthesia. Never receiving what he felt to be his due, Morton died an embittered man. Charles Jackson, Morton's chemistry teacher at Harvard, also claimed
priority in the discovery; it was he who had suggested that Morton use pure
sulfuric ether. WILLIAM T. G. MORTON Inventor and Revealer of Anaesthetic Inhalation Before Whom, in All Time, Surgery Was Agony By Whom Pain in Surgery Was Averted and Annulled Since Whom Science Has Control of Pain Anesthesia after 1846 Although it is rarely used today, ether was the ideal 'first' anesthetic. Chemically, it is readily made in pure form. It is relatively easy to administer, since it is a liquid at room temperature but is readily vaporized. Ether is potent, unlike nitrous oxide, and thus a few volumes percent can produce anesthesia without diluting the oxygen in room air to hypoxic levels. It supports both respiration and circulation, crucial properties at a time when human physiology was not understood well enough for assisted respiration and circulation to be possible. And ether is not toxic to vital organs. The next anesthetic to receive wide use was chloroform. Introduced by
the Scottish obstetrician James Simpson in 1847, it became quite popular,
perhaps because of its more pleasant odor. Other than this and its
nonflammability, there was little to recommend it (Sykes, 1960). The drug is
a hepatotoxin and a severe cardiovascular depressant. Despite the relatively
high incidence of intraoperative and postoperative death associated with the
use of chloroform, it was championed, especially in The course of anesthesiology in the Other Anesthetic Agents Nitrous oxide fell into disuse after the apparent failure in The anesthetic properties of cyclopropane were accidentally discovered
in 1929, when chemists were analyzing impurities in an isomer, propylene.
After extensive clinical trial at the The skeletal muscle relaxants (neuromuscular blocking agents) also were discovered and their pharmacological properties demonstrated long before their introduction into clinical practice. Curare, in crude form, had long been used by South American Indians as a poison on their arrow tips (see Chapter 9: Agents Acting at the Neuromuscular Junction and Autonomic Ganglia). Its first clinical use was in spastic disorders, where it could decrease muscle tone without compromising respiration excessively. It was then used to modify the violent muscle contractions associated with electroconvulsive therapy of psychiatric disorders. Finally, in the 1940s, anesthesiologists used curare to provide the muscular relaxation that previously could be obtained only with deep levels of general anesthesia. Over the next half-dozen years several synthetic substitutes were used clinically. It is difficult to overemphasize the importance of muscle relaxants in anesthetic practice. Their use permits adequate conditions for surgery with light levels of general anesthesia; cardiovascular depression is thus minimized, and the patient awakens promptly when the anesthetic is discontinued. Although the desirability of an intravenous anesthetic agent must have been apparent to physicians early in the twentieth century, the drugs at hand were few and unsatisfactory. The situation changed dramatically in 1935, when Lundy demonstrated the clinical usefulness of thiopental, a rapidly acting thiobarbiturate. It was originally considered useful as a sole anesthetic agent, but the doses required resulted in serious depression of the circulatory, respiratory, and nervous systems. Thiopental, however, has been enthusiastically accepted as an agent for the rapid induction of general anesthesia. Various combinations of intravenous drugs from several classes have been used recently as anesthetic agents, usually together with nitrous oxide. The administration of short-acting opioids by constant intravenous infusion (with little or no potent inhalational agent) is an exciting current development in the practice of anesthesia. |
Modern Anesthesiology
|
What Is Anesthesia? The answer to this question is both more complex and more elusive than generally appreciated. To guide the discussion we may first consider the basic goals of anesthesia, namely to create a reversible condition of comfort, quiescence, and physiological stability in a patient before, during, and after performance of a procedure that would otherwise be painful, frightening, or hazardous. This statement embodies concepts that have evolved with modern developments within the specialty of anesthesiology that were not necessarily envisioned by early workers. After the public demonstration of diethyl ether in 1846, anesthesia was eagerly embraced by the general public and the medical profession even as complications associated with its use were noted with concern (Codman, 1917). For several decades, the dramatic increase in surgical procedures performed was tracked precisely by increases in the deaths and major morbidities attributed to the anesthesia (Sykes, 1960). Foremost among the complications were regurgitation and aspiration of stomach contents and cardiovascular collapse, now thought to be disturbances of heart rhythm resulting from an interaction between direct effects of the agents that were used with the physiological response to surgical stress. To realize fully the benefits and the promise of anesthesia, laboratory and clinical researchers have investigated the pharmacological and physiological actions of potent new therapeutic agents, guided development of monitoring equipment and drug-delivery devices, and created advanced techniques and principles of practice (Wiklund and Rosenbaum, 1997). Recent refinements have included progressive attention to issues of risk assessment and risk reduction. Unlike the practice of every other branch of medicine, anesthesia usually is considered to be neither therapeutic nor diagnostic. The notable exceptions to this, including treatments of status asthmaticus with halothane and intractable angina with epidural local anesthetics (and other examples), should not obscure the critical point, which permeates the training and practice of the specialty. Patients present for surgery with an array of medical conditions both known and unknown, while ingesting drugs that alter cardiovascular and other responses. They will then undergo a series of physiological stressors from which they must be protected, including effects of the very agents used to initiate and sustain the anesthetic condition. Reduction of complications may be separated for illustrative purposes into three categories:
The Surgical Stress Response The stress of surgery includes (presumably) adaptive responses involving three systems, the hypothalamic-pituitary-adrenal axis, the sympathetic nervous system, and the acute-phase response, all of which may be activated by psychological stress, tissue injury, intravascular volume changes, anesthetic agents, pain, and organ manipulation (Udelsman and Holbrook, 1994). These stimuli trigger a cascade of neurohumeral responses, including increases in cortisol, catecholamines, heat shock proteins, and cytokines which, in turn, provoke tachycardia, hypertension, increased metabolism, hypercoagulability, and decreased immune function (Breslow, 1998). Specific associated morbidities include myocardial ischemia and infarction (Mangano et al., 1996), arrhythmias (Balser et al., 1998), thrombosis, infection, and delayed wound healing. The effects of anesthesia attenuate some components of the surgical stress response. In addition to promoting stability within the clinical milieu described above, it should be emphasized that the kinetics of anesthetic agents and the techniques used must conform to certain time constraints so that the duration and depth of anesthetic states parallel the tempo of the surgical procedure. Hence the uptake, distribution, and elimination of anesthetic drugs are important matters, and the discovery of agents with rapid onset and elimination has greatly improved this aspect of care. The rest of this chapter will be organized around discussions of the functionally separable time periods: before (preoperative), during (intraoperative), and after (postoperative) surgery, illustrating within each period the principles of perioperative medical care and the anesthesia-specific issues as they logically appear. |
Preoperative Period
|
Anesthetic considerations prior to surgery include patient evaluation and the administration of medications that treat chronic or acute disease and that facilitate the impending anesthetic experience. Preexisting comorbidities are important determinants of perioperative risk. Risk prediction indices or algorithms have been developed (Goldman et al., 1977; Palda and Detsky, 1997) that incorporate several pathophysiological conditions, including known or probable coronary artery disease; electrocardiogram (ECG) changes; signs and symptoms of congestive heart failure; abnormalities indicating pulmonary, renal, or hepatic disease; patient age; and invasiveness of the planned surgical procedure. Each one of these conditions has one or more treatment options that have been developed to neutralize its effect and prevent it from worsening during or after the procedure. This is a major feature of the practice of anesthesiology. Decisions are made with regard to the techniques employed, agents chosen, and monitors used based on the preoperative information (Sweitzer, 2000). Depending on the patient's condition, interventions suggested by the preoperative evaluation range from preoperative coronary angiography (with balloon angioplasty or coronary artery bypass grafting in appropriate cases) (Eagle et al., 1996), optimization of cardiac loading conditions guided by data from pulmonary artery catheters prior to surgery (Berlauk et al., 1991), simple corrections of electrolyte and hemoglobin abnormalities, and institution of antihypertensive therapy. Novel proposals for preoperative assessment are emerging from modern techniques of molecular biology. Genetic polymorphisms, the discovery of which has been accelerated as a consequence of the mapping of the human genome, are being linked to medical conditions (hypertension, coagulation disorders, arrhythmias) and variable responses to therapy. The challenge now is to apply these same concepts to the surgical environment. Preoperative evaluation and risk assessment may evolve to include broad screenings for polymorphism associated with morbidity and, thereby, guide risk-reduction therapies. Preoperative Medication Chronic Medications Preoperative medication begins with virtually all of the patient's normal daily morning doses of significant drugs. This includes inotropic, chronotropic, dromotropic, and vasoactive agents, especially antihypertensive agents. Diuretics are controversial, as are metformin and monoamine oxidase inhibitors. The latter agents have serious interactions with meperidine and other drugs used during surgery, but these interactions can be managed. The management of insulin-dependent diabetes and chronic steroid use is addressed formally by protocols. Patients dependent on drugs that are associated with withdrawal symptoms must be given special treatment. The importance of maintaining cardiovascular medications is
illustrated by clinical studies showing that the incidence and severity of
myocardial ischemia is associated with elevated heart rates in the
postoperative period. This finding led to clinical trials of prophylactic,
perioperative administration of Other preoperative medications are used to treat conditions directly related to anesthetic issues that may arise before, during, and after surgery. Anticholinergic Drugs Though previously widely employed for their vagolytic and membrane-drying properties, anticholinergic agents (see Chapter 7: Muscarinic Receptor Agonists and Antagonists) are little used, preoperatively, in adults in modern practice, except in specific situations requiring reduced secretions. Vagotonia may occur intraoperatively from increases in ocular pressure, visceral traction, and other reasons, and it is treated by interrupting the stimulus temporarily while administering anticholinergic drugs. Drugs That Reduce the Acidity and Volume of Gastric Contents The induction of general anesthesia eliminates the patient's ability to protect the airway should regurgitation of stomach contents occur. This is why nothing-by-mouth ('npo') status is emphasized so strongly for patients having elective procedures. Decreasing the volume of gastric contents further reduces the likelihood of regurgitation, and increasing the gastric pH above 2.5 reduces damage to the lungs in the event of aspiration. Histamine H2-receptor antagonists, antacids, and prokinetic agents (see Chapters 37 and 38) frequently are administered to achieve these conditions. Sedative-Hypnotics and Antianxiety Agents Drugs such as benzodiazepines and butyrophenones (see Chapter 17: Hypnotics and Sedatives) are useful when administered before surgery both for patient comfort and for facilitation of the anesthetic state. When given in conjunction with opioids, there is reduction of catecholamine release in response to surgical stimuli (Newman and Reves, 1993). Opioids Opioids (see Chapters 14: General Anesthetics and 23: Opioid Analgesics) may be used preoperatively in small doses to act synergistically with sedatives in creating a tranquil patient. Only in persons actually having pain or experiencing incipient withdrawal symptoms are they specifically indicated before surgery. |
Intraoperative Period
|
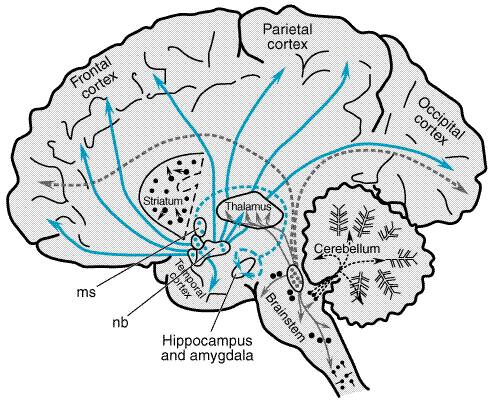
Monitoring Standard monitoring (Pierce, 1989) during anesthesia includes continuous electrocardiography, monitoring of heart rate and body temperature, pulse oximetry, and capnography (the measurement of carbon dioxide concentration in exhaled gas) and frequent noninvasive blood pressure measurement. Additional parameters measured may include urine output, blood loss, and ventilation-related parametersincluding inspired oxygen, tidal volume, minute ventilation, peak inspired airway pressure, and all gas flows. Direct measurement of inspired and expired levels of volatile anesthesic agents is desirable. In selected cases, invasive measurements are made of arterial pressure, central venous pressure, pulmonary artery pressure, cardiac output, pulmonary capillary wedge pressure, right ventricular ejection fraction, and pulmonary artery oxygen saturation. Transesophageal echocardiography has proven to be most useful in cardiac surgery and in other special situations. General Anesthesia There are two fundamentally different ways of achieving the basic anesthetic conditions required to perform surgical procedures, general anesthesia and regional (or conduction) anesthesia. The hallmark of general anesthesia is loss of consciousness as represented by the historical vignette and the description 'going to sleep,' which continues to be used by lay persons and professionals alike. Regional anesthesia is effected by the injection or infiltration of certain amides or esters that block signal conduction (usually voltage-gated sodium channels) near nerves either peripherally or more centrally (see Chapter 15: Local Anesthetics). This widely used technique has advantages (including intense attenuation of noxious stimuli) as well as drawbacks, as discussed in a later section of this chapter. General anesthesia is classically described by four qualities: hypnosis (usually meaning sleep or loss of consciousness), amnesia, analgesia, and muscle relaxation. To these must be added the broader concepts of maintaining physiological stability, attenuation of the surgical stress response, and a host of techniques to lessen the aforementioned categories of risk. The intraoperative period for general anesthesia is normally broken down into three phasesinduction, maintenance, and emergenceeach with its special considerations. Induction The 'induction' of general anesthesia occurs when a conscious or otherwise responsive being is rendered unconscious by the effects on the nervous system of inhaled or intravenously injected agents. Loss of Consciousness Oddly, after 150 years of investigation, researchers still do not know with certainty either the molecular mechanisms whereby general anesthetic agents exert their neurological effect or the brain structures or circuitry involved in the loss of consciousness. It may be disconcerting, but a corollary of this lack of understanding is that assessment of the 'depth' of anesthesia must be determined by indirect means (i.e., changes in vital signs) that are only variably reliable. The variety of structurally diverse molecules that can create the condition we call general anesthesia is astonishing (see Chapter 14: General Anesthetics). The group includes volatile organic agents (halogenated hydrocarbons, diethyl ether, chloroform); inorganic gases such as nitrous oxide and xenon; alcohols; and an array of intravenous agents, including barbiturates, etomidate, propofol, and ketamine. Exactly how and precisely where anesthetic agents produce their remarkable effects have been under investigation for a century (Meyer, 1899, 1901; Overton, 1901). At the cellular level, fundamental discoveries in the last decade have greatly changed traditional concepts that attributed anesthetic action to nonspecific membrane solubility of anesthetic molecules with resulting perturbed structural and dynamic properties of the lipid membrane. Recent work has identified functional targets for a wide range of intravenous and inhalational anesthetic molecules. These primarily include ligand-gated ion channels, such as the gamma-aminobutyric acid type A (GABAA), glycine, 5-HT3 serotonin, nicotinic acetylcholine (ACh), and subtypes of glutamate receptors (NMDA, AMPA, and kainate) (see Chapters 12: Neurotransmission and the Central Nervous System and 14: General Anesthetics). GABAA and glutamate receptors are found throughout the brain, while ACh and serotonin receptors are associated with specific pathways of interconnecting nuclei. Identifying the location of these receptors in the central nervous system (CNS), the function of pathways that incorporate them, and the behavioral and physiological changes induced by their interaction with anesthetic molecules are some of the fundamental challenges to modern research. Any discussion of loss of consciousness immediately begs the question: What is consciousness? Descriptions include the qualities of perception, attention, volition, self-awareness, and memory. Purposeful movement and response to auditory, tactile, or noxious stimulation classically have suggested consciousness, but the role of spinal cord reflexes complicates this idea. Consciousness has been dubbed a 'prescientific' concept (Kulli and Koch, 1991), but it is enjoying a resurgence of attention from a range of investigators from philosophers to molecular biologists (Crick and Koch, 1998; Chalmers, 1996). Neural Correlates of Consciousness Two components of conscious awareness have been proposed: 'arousal-access-vigilance' and 'mental experience-selective attention' (Block, 1996). Crick and Koch (1995) postulate that some identifiable, active neuronal processes in the brain are associated with states of awareness. The quest is to determine what is special, if anything, about their connections and manner of activation. Such circuitry would be called the 'neural correlates of consciousness' (Crick and Koch, 1998), and work is in progress to establish the concept's validity using in vivo imaging, single neuronal types, and intracellular components. Several observations suggest that neural pathways mediated by ACh control both the content of conscious awareness and its level of intensity (Perry et al., 1999). Mental disturbances seen with degenerative brain diseases include fluctuating levels of conscious awareness and are associated with deficits in neocortical ACh systems (Perry and Perry, 1995). The cholinergic system is distributed in various nuclei (Figure 131), including two major groupsthe basal forebrain and pedunculopontine nuclei with extensive bidirectional connections to the cortex and thalamus. These are considered to be essential for controlling selective attention (Bentivoglio and Steriade, 1990). The extent of cholinergic projections from the nucleus basalis to the human cortex suggests a major role in regulatory modulation. Continuous firing during rapid-eye-movement (REM) sleep is sufficient to activate the cortex (Perry et al., 1999). The phenomenon of brain stem activation of cortical processes (accepted as necessary for consciousness as defined in higher animals) has received attention, because the midbrain reticular formation (MRF) has neural projections from brainstem to thalamic nuclei to cortical structures, and the main neurotransmitters (ACh and glutamate) have been described (Steriade, 1996). Note that either ACh receptors or glutamate receptors or both are inhibited by a wide range of anesthetic agents including the volatile agents, barbiturates, and ketamine (Krasowski and Harrison, 1999).
In human beings engaging in tasks that require alertness and attention, there is increased blood flow in the MRF (Kinomura et al., 1996). Stimulation of the MRF in anesthetized animals causes changes in the cortical EEG to resemble the awake state. Finally, Shimoji et al. (1984) have shown that the excitatory responses of MRF neurons, evoked by somatosensory stimulation in cats, are suppressed by anesthetic agents from several classes, while inhibitory responses of the MRF neurons are potentiated by barbiturates and ether. It has been proposed that awareness uses a serial attention mechanism consisting of high-frequency (40-Hz), synchronized oscillations that transiently 'bind together' widely distributed cortical neurons related to different aspects of a perceived object (color, size, motion, sound, etc.) (Crick and Koch, 1990; Steriade et al., 1996). Direct application of ACh induces just such fast synchronized activity in hippocampal slice preparation (Fisahn et al., 1998). Again, ACh receptors are inhibited by halogenated agents, barbiturates, and ketamine (Perry et al., 1999). It has been suggested that the thalamus is the most likely source of this oscillatory activity because of its extensive bidirectional connections with higher and lower structures. It seems likely that the action of ACh in the cortex and thalamus is central to the normal maintenance of conscious awareness, as are interactions among ACh, GABA, and glutamate, all three of which control the cholinergic neurons in the basal forebrain and pedunculopontine projections. Other pathway candidates for neural correlates of consciousness
include noradrenergic projections from pontine locus ceruleus nuclei, which
distribute axons cephalad to the dorsal thalamus, hypothalamus, cerebellum,
forebrain, and neocortex. Not only does this system contain 50% of all
noradrenergic cells in the brainstem, but changes in concentrations of norepinephrine
alter anesthetic dose requirements (Angel, 1993). Hemodynamic Effects The physiological effects of anesthesia induction associated with the majority of both intravenous and inhalational agents include most prominently a decrease in systemic arterial blood pressure. The cause is either direct vasodilation or myocardial depression or both, a blunting of baroreceptor control, and a generalized decrease in central sympathetic tone (Sellgren et al., 1990). Agents vary in the magnitude of their specific effects (see Chapter 14: General Anesthetics), but in all cases the hypotensive response is enhanced in the face of underlying volume depletion, intrinsic depressed myocardial function, and cardiovascular medications. Even anesthetics that show minimal hypotensive tendencies under normal conditions (etomidate, ketamine) must be used with caution in trauma victims, in whom intravascular volume depletion is being compensated by intense sympathetic discharge. Smaller than normal induction dosages are employed in patients presumed to be sensitive to hemodynamic effects of anesthetics (e.g., elderly or debilitated patients, those with systolic and diastolic dysfunction, those taking diuretics or who have had recent dye studies or preparation for bowel surgery). Administration of direct- and indirect-acting sympathomimetics (see Chapter 10: Catecholamines, Sympathomimetic Drugs, and Adrenergic Receptor Antagonists) will contribute to stability. Also, it is common to administer intravenous fluids liberally prior to and during induction to avoid hypotension. In some cases, fluid is relatively contraindicated, requiring the use of inotropic agents and/or vasoconstrictors to support the circulation. Airway Maintenance Airway maintenance is essential following induction. Ventilation must be assisted or controlled for at least some period and perhaps throughout surgery. The gag reflex is lost, and the stimulus to cough is blunted. Lower esophageal sphincter tone is reduced. Both passive and active regurgitation may occur. Endotracheal intubation was introduced in the early 1900s (Kuhn, 1901) and was a major reason for a decline in the number of aspiration deaths. Muscle relaxation is valuable during the induction of general anesthesia where it facilitates management of the airway including endotracheal intubation. Neuromuscular blocking agents are commonly used to effect such relaxation (see Chapter 9: Agents Acting at the Neuromuscular Junction and Autonomic Ganglia). Endotracheal intubation both prevents aspiration and permits control
of ventilation. While the procedure is used broadly, there also are
alternative procedures. In patients who have had nothing to eat and are
without symptoms of reflux, maintenance of ventilation (usually
assisted-spontaneous) with an externally applied mask has been common for
certain procedures not requiring muscle relaxation. It is important to note that
the combination of direct laryngoscopy and intubation are stimuli fully
comparable to an abdominal incision. Instrumentation of the subglottic airway
stimulates secretions and exacerbates bronchospastic reactions as well, so
when feasible, it might be desirable to avoid the procedure. An instrument
called the laryngeal mask airway (Brain, 1983) has been progressively
employed. This device consists of a flexible oval fenestrated diaphragm that
is inserted blindly into the oropharynx. When seated, the diaphragm covers
the laryngeal opening and can be sealed by inflation of a balloon around its
circumference. Use of the laryngeal mask is becoming very popular; more than
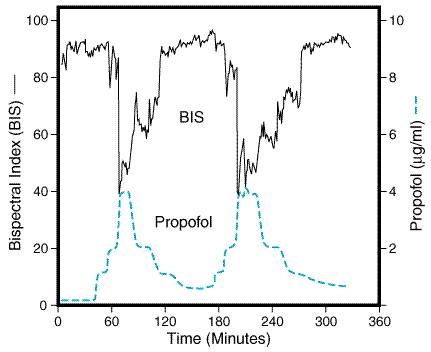
half of the anesthetics administered in Stabilizing the Following induction, continued management of the patient may be associated with fluctuations in blood pressure under the competing influences of anesthetic-induced depression and surgical stimulation. Part of the art and science of administering anesthetics is learning to manage the process smoothly, matching metabolic demands with appropriate oxygen supply while ensuring unconsciousness in preparation for the impending surgical stimulation, which will continue (not necessarily uniformly) throughout the case. Assessing the patient's level of consciousness, assuring adequate depth of anesthesia, and minimizing recall obviously are central to the goals of general anesthesia. Signs and Stages of Anesthesia Between 1847 and 1858, John Snow described certain signs that helped him determine the depth of anesthesia in patients receiving chloroform or ether. In 1920, Guedel, using these and other signs, outlined four stages of general anesthesia, dividing the third stagesurgical anesthesiainto four planes. The somewhat arbitrary division is as follows: I, stage of analgesia; II, stage of delirium; III, stage of surgical anesthesia; IV, stage of medullary depression. Although the classical signs and stages of anesthesia are partly recognizable during administration of volatile anesthetics, they are most often obscured by modern anesthetic techniques. Intravenous induction agents (thiopental, etomidate, propofol) produce a deep plane of anesthesia virtually within one circulation time, while certain properties of new inhalational agentssuch as low blood solubility (desflurane) and minimal airway irritability (sevoflurane)allow for such rapid establishment of anesthesia that the transition to unconsciousness is almost immediate. Furthermore, Cullen and coworkers (1972) demonstrated that no single one of the major signs described by Guedel correlated satisfactorily with the measured alveolar concentrations of anesthetic during prolonged, stable states. Thus, only the term stage two remains in common use today, signifying a state of delirium in the partially anesthetized patient most frequently seen during emergence from anesthesia where volatile inhalational agents have been used. Maintenance The maintenance phase of general anesthesia is associated with changes in intensity of stimulation, fluid shifts (third spacing), blood loss, acid-base disturbances, hypothermia, coagulopathies, and other conditions. Of course, in many cases none of these things occurs, but special measurements, monitors, and precautions are necessary when they door in their anticipation. Management of the anesthetic interplays constantly with the general physiology of the patient. Historically, and continuing to the present, the great majority of cases involves the administration of one or more of the anesthetic gases during the maintenance phase. Special factors govern the transport of anesthetic molecules from inspired gas through the lungs to blood and then to the brain, including (1) concentration of the anesthetic agent in inspired gas, (2) pulmonary ventilation delivering the anesthetic to the lungs, (3) transfer of the gas from the alveoli to the blood flowing through the lungs, and (4) loss of the agent from the arterial blood to all the tissues of the body. Obviously, the concentration in neural tissues is of greatest importance. The details of the uptake and distribution of anesthetic agents are covered in Chapter 14: General Anesthetics. With full cognizance of the factors related to the delivery of anesthetic gases to the brain, there remains the need to characterize and quantify the relative potencies of volatile anesthetic agents in a practical way. The Minimum Alveolar Concentration (MAC) Since 1965, the relative potencies of volatile anesthetic agents (halothane, enflurane, isoflurane, etc.) and N2O and xenon have been described by the concentration (minimum alveolar concentration or MAC) that renders immobile 50% of subjects exposed to a strong noxious stimulation (1.0 MAC) (Eger et al., 1965), such as surgical incision. Lack of movement in response to incision has been assumed to imply unconsciousness and amnesia in an unparalyzed patient. A major strength of this concept stems from the facts that the concentration of anesthetic gases can be measured and displayed in each breath and that the end-tidal expired partial pressures approximate the brain concentration. The latter assumption fails during periods of rapid change. Also useful is the fact that doses of different agents expressed as MAC equivalents appear to be additive (Cullen et al., 1969; Miller et al., 1969). In human beings exposed to modern inhalational agents, mild analgesia begins at about 0.3 MAC; amnesia is present at 0.5 MAC, where the patient can respond to command or even speak but does not recall this later (Levy, 1986). Obtundation deepens with 1.0 MAC where (by definition) 50% of patients remain immobile after stimulation. At higher doses (about 1.3 MAC), the sympathetically mediated response to surgery is blunted (Roizen et al., 1981). Doses of inhalational agents higher than 2.0 MAC (equilibrated) are said to be potentially lethal, but in fact, such MAC multiples using balanced combinations of inhalational and intravenous agents are commonly achieved and sustained without untoward effect. Pharmacological support of the circulation may be required. Obviously, a similar concept exists for intravenous anesthetics (barbiturates, propofol, etomidate) and adjuvants, but there is currently no on-line, real-time measurement of blood drug concentration for these compounds. The clinician must rely on body weight and age-adjusted dose guidelines to approximate the target blood levels, and then adjust the delivery rates according to various physiological responses, notably changes in blood pressure and heart rate. Knowledge of the MAC fraction or multiple does not necessarily convey all of the necessary information. The anesthesiologist needs to assess both the level of responsiveness that exists at a point in time (with the level of stimulation existing at that moment) and the likelihood that the patient will react to an anticipated increase in the stimulation (such as laryngoscopy, incision, use of a retractor). As surgery proceeds, continuous adjustments in the delivery rates of both inhalational and intravenous agents are required in an attempt to ensure unconsciousness, amnesia, immobility, and analgesia while simultaneously attending to the drifting physiological conditions. Limitation of MAC It is important to note that the concept of MAC leaves 50% of patients who actually move with stimulation and who thereby fail one measure of lack of awareness. While the dose-response curve is steep with 99% of subjects immobile at 1.3 MAC, the possibility of awareness and recall still may exist. Moreover, movement itself is of no use in the large number of patients who receive muscle relaxants. Other indicators of awareness that are independent of muscle relaxation include lacrimation, diaphoresis, and pupillary dilation. These signs are highly suggestive if they are present, but their absence is not definitive. While the absence of movement does not ensure unconsciousness, neither does its presence necessarily imply consciousness. Elegant experiments with laboratory animals using EEG and MRF recordings that split the circulation between the brain and torso show that 1.0 MAC of isoflurane delivered to both circulations largely suppressed both EEG and MRF responses to noxious stimuli delivered to the torso. However, there were marked effects when the torso concentration was lowered to 0.3 MAC while the brain remained at 1.0 MAC (Antognini et al., 2000). The animals moved with torso stimulation although the brain remained unconscious by EEG criteria. It has been appreciated for some time that spinal cord effects are important in general anesthesia (Kendig, 1993). Indeed, subarachnoid injection of local anesthetics lowers the dose of sedative required to achieve a hypnotic response (Ben-David et al., 1995). These observations explain the long-noted clinical experience that a patient who moves with incision is not necessarily 'awake' and one who does not move is not necessarily unconscious or amnesic. The experimental validation of this phenomenon clearly calls into question the applicability of MAC as classically defined and sets the stage for new efforts to better assess brain states during anesthesia. Amnesia Memory processes associated with anesthesia and surgery are complex (Bailey and Jones, 1997). Both explicit (free recall) memory and implicit (subconscious) phenomena are described. The latter may be identified by tests such as category generation, free association, and forced choice recognition. Recent large studies have suggested that the incidence of explicit recall is 0.15% following general anesthesia (0.18% when using muscle relaxants, 0.10% without muscle relaxants) in patients undergoing surgery and anesthesia when interviewed three times following the case (Sandin et al., 2000). Interestingly, the incidence of recall was unaffected by the use of preoperative benzodiazepines. Since many millions of anesthetic procedures are performed each year, thousands of people actually will experience intraoperative awareness. Further, it is well established (Schwender et al., 1998) that delayed neurotic symptoms (posttraumatic stress disorder) can follow awareness during general anesthesia. Monitoring Consciousness The search for a monitor of level of consciousness or anesthetic depth obviously has centered on electroencephalography (and evoked potentials). Whereas the processed EEG power spectrum median frequency falls from about 10 Hz in the awake state to 5 Hz or less in both natural sleep and anesthesia in the absence of verbal stimuli, it does so only for some agents, and it can be altered further by hypoxia, hypocarbia, hypothermia, and other common conditions during surgery (Jessop and Jones, 1992). The volatile agents, as previously noted, elicit an excitement phase registered by the EEG as high frequency and high power transiently, as the subject passes through the planes of anesthetic depth. The EEG has been deemed unreliable as a measure of anesthetic dose or as a predictor of awareness or recall (Levy, 1986). Recent developments have changed that impression. Highly processed EEG signals have evolved from first order (signal amplitude mean and variance) to second order (power spectrum) and now to higher order statistics. The latter include the bispectrum and trispectrum (third- and fourth-order statistics, respectively) (Rampil, 1998). Special attention is focused on the bispectrum, which measures the correlation between phase and frequency components. Four derived subparameters have been defined and combined through weighting factors, determined empirically to produce a dimensionless number, called the bispectral index or BIS (Aspect Medical Systems, Inc., Natick, MA), which varies from 0 to 100. The proprietary algorithms, which give rise to the BIS value, have evolved by incorporating data from thousands of patients undergoing anesthesia with agents from different classes. A monitor receives signals from electrodes placed on the forehead and displays the BIS value continuously. Table 131 shows the experimentally derived correlation between absolute value and effect. Figure 132 shows the hypnotic level (BIS) versus time in a volunteer receiving a propofol infusion demonstrating a direct relationship between blood level of the hypnotic drug and level of consciousness. This technology has become available at a time of growing international concerns regarding intraoperative awareness (Ghoneim, 2000). It must be emphasized that the ability of the device to assure lack of consciousness or recall has not been established, but recall below a reading of 60 apparently has not been reported.
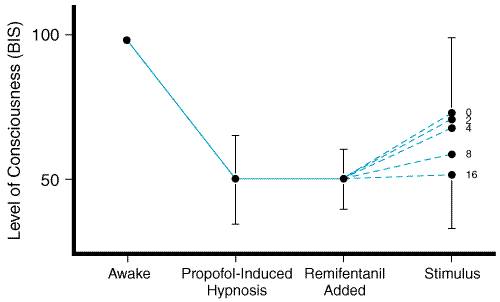
Analgesia Although inhalational anesthetic agents have an analgesic component in that the response to noxious impulses are blunted, this is mild at low doses and is only effective for surgery at higher concentrations (1.3 MAC or greater) where other side effects may be limiting. Most general anesthetics employ some dose of an opioid to provide analgesia. Opioids Opioids have been used for centuries for their analgesic properties. The identification of opioid receptors in the spinal cord (Kitahata et al., 1974) and brainstem, and the manufacture of synthetic opioids of great potency (fentanyl, alfentanil, sufentanil) have transformed the practice of anesthesia over the past 30 years. The pharmacology of opioids is covered in Chapters 14: General Anesthetics and 23: Opioid Analgesics. Opioids are synergistic with sedative-hypnotic agents and inhalational agents, including nitrous oxide. The ability of opioids to block painful stimuli, accompanied by intrinsic hemodynamic stability, has led to so called 'high-dose' techniques, notably for cardiac surgery (a maximal stimulus). In this approach, opioids are combined only with an amnesic agent such as midazolam (Curran, 1986), since the opioid doses that cause autonomic stability (and lack of movement) will not reliably cause loss of consciousness or amnesia (Ausems et al., 1983). More common is the use of lower doses of opioids administered continuously or intermittently during surgery in conjunction with a volatile general anesthetic, the latter given in fractions of MAC (0.5 to 0.8), and nitrous oxide, where not contraindicated. This combination, called 'balanced anesthesia' by some, permits sustaining unconsciousness (presumably) with the volatile anesthetic while supplying analgesia with opiates for the duration of surgery and into the postoperative period. Return to responsiveness at surgery's end can be prompt. The introduction of remifentanil, an ester opioid metabolized by plasma esterases, has created a new dimension for intensity of analgesia during surgery and for rapid awakening during recovery. This agent is not only intrinsically very potent, but it has a very short half-life, allowing for higher infusion rates during the intense periods of stimulation (Brkle et al., 1996). Contribution of Analgesia to the To separate the influences of analgesia and hypnosis on anesthetic
requirements in conditions of variable stimulation, we consider a study of
patients who received an infusion of the hypnotic propofol in a dose
predicted to induce marked loss of consciousness (blood level 4
The methodology in this study illustrates an alternative technique for managing general anesthesia with only intravenous agents. Called TIVA, for total intravenous anesthesia, it frequently incorporates an amnesic drug such as midazolam to ensure lack of recall (Newman and Reves, 1993) and a muscle relaxant in addition to analgesic and hypnotic agents. The ability to assess levels of consciousness objectively enhances the appeal of TIVA. The technique may increase in popularity, especially if the cost of the newer, shorter-acting agents can be justified. Muscle Relaxation The fourth quality of general anesthesia is muscle relaxation. This, at least, implies that patients should not move with incisionan achievable goal with sufficient doses of inhalational anesthetics, intravenous anesthetics, opioids, or some combination. However, following the need for brief muscle paralysis to achieve intubation, more prolonged relaxation is required for some orthopedic, general abdominal, and otolaryngology surgeries. Muscle relaxants are further discussed in Chapters 9: Agents Acting at the Neuromuscular Junction and Autonomic Ganglia and 14: General Anesthetics. Their usual, ready reversal by cholinesterase inhibitors (e.g., neostigmine; see Chapter 8: Anticholinesterase Agents), along with development of drugs with a wide range of half-lives, has made use of muscle-relaxant drugs widespread in surgery. Emergence As surgical stimulation begins to lessen during wound closure, delivered doses of anesthetic agents will be reduced in a manner that reflects their specific pharmacokinetics. Both inhaled and intravenous drugs can exhibit delayed dissipation caused by either slow washout (from poorly perfused fat-rich tissue) or by the character of their distribution and metabolism. The major factors that affect rate of elimination of inhaled anesthetics are the same as those that are important in the uptake phase: pulmonary ventilation, blood flow, and solubility in blood and tissue. Because of the high blood flow to brain, the tension of anesthetic gas in the brain decreases rapidly, accounting for the rapid awakening from anesthesia noted with relatively insoluble agents such as nitrous oxide (see Chapter 14: General Anesthetics). The physiological changes accompanying emergence from general anesthesia can be profound. Hypertension and tachycardia are common as the sympathetic nervous system regains its tone and is enhanced by pain (Breslow, 1998). Myocardial ischemia can appear or markedly worsen during emergence in patients with coronary artery disease. Emergence excitement occurs in 5% to 30% of patients and is characterized by tachycardia, restlessness, crying, moaning and thrashing, and various neurological signs (Eckenhoff et al., 1961). Postanesthesia shivering occurs frequently because of core hypothermia, which was common before modern realization of its negative effects. A small dose of meperidine (12.5 mg) lowers the shivering trigger temperature and effectively stops the activity. The incidence of all of these emergence phenomena is greatly reduced when opioids are employed as part of the intraoperative regimen. Hypothermia Patients develop hypothermia (body temperature <36C) during surgery for several reasons, including low ambient temperature (and exposed body cavities), cold intravenous fluids, altered thermoregulatory control, and reduced metabolic rate. General anesthetics lower the core temperature set point, at which thermoegulatory vasoconstriction is activated to defend against heat loss. Further, vasodilation caused by both general and regional anesthesia blocks the normal thermal constriction, thereby redistributing heat in the body mass and leading to a rapid decline in core temperature until the new (lower) set point is reached (Sessler, 2000). Total body oxygen consumption decreases with general anesthesia by about 30%, and thus heat generation is reduced. Even small drops in body temperatures may lead to an increase in perioperative morbidity, including cardiac complications (Frank et al., 1997), wound infections (Kurz et al., 1996), and blood loss. Prevention of hypothermia has emerged as a major goal of anesthetic care. Modalities to maintain normothermia include using warm intravenous fluids, heat exchangers in the anesthesia circuit, forced-warm-air covers, and new technology involving water-filled garments with microprocessor feedback control to a core temperature set point. Regional (Local) Anesthesia Local anesthetics include esthers (e.g., cocaine, procaine, tetracaine) and amides (e.g., lidocaine, bupivicaine, ropivicaine) that are injected in the vicinity of nerves to cause temporary, virtually complete interruption of neural traffic (see Chapter 15: Local Anesthetics), enabling surgery to proceed in comfort. Upper limb procedures may be facilitated by plexus blockade, while surgery on the thorax, abdomen, and lower extremities may be accomplished by neuraxial blockade (epidural and spinal), either in conjunction with general anesthesia or as the sole modality employed. Spinal anesthesia, first performed in 1889 (see Wulf, 1998) is effected by injection of local anesthetic agents into the lumbar (L34, L45) subarachnoid cerebrospinal fluid. Since the spinal cord rarely extends below L2, the injection needle harmlessly pushes aside the strands of the cauda equina. Depending on the volume of injectate (usually 1 to 3 ml), specific gravity (may be either hyper-, hypo-, or isobaric, varying with the diluent), manner of injection, and the position of the patient, spinal blockade may extend from T2 down through the sacral roots. Epidural anesthesia proceeds with injection of a volume (10 to 25 ml) of local anesthetic solution into the epidural 'potential' space. Because dural puncture is not intended, the site of entry may be at any vertebral level permitting a band of 'segmental' blockade approximately limited to the region of interest. Spinal and epidural anesthesia share many similarities and will be discussed together as 'neuraxial' techniques with specific differences highlighted. The sympathetic nervous system is mediated through spinal segments T1L2, and neuraxial blockade will most commonly involve several of these. The drop in blood pressure that ensues is anticipated and compensated for, as necessary, with fluid administration and vasopressor agents. In volume-depleted patients, aggressive prophylactic measures are taken. Arterial and venous dilation cause most of the pressure drop, but cardiac sympathetic nerves emerge from T1T4 and also may be blocked. This blockade of sympathetic nerves going to the heart is used to advantage in the treatment of myocardial ischemia refractory to conventional medical therapy by administering a thoracic epidural injection of a local anesthetic agent (Blomberg et al., 1989). Further, the decrease in afterload seen with all levels of neuraxial blockade can improve cardiac output in patients with congestive heart failure. To achieve neuraxial blockade over a prolonged period (more than 3 hours), a catheter is placed in either the subarachnoid or epidural space for either bolus injection or continuous infusion. This allows continuance of neural blockade into the postoperative period. As previously noted, regional anesthesia may have special advantages over
general anesthesia, including attenuation of the surgical stress response.
Intense blockade using regional anesthesia can hold intraoperative
catecholamines to presurgical values (Breslow et al., 1993). There is
evidence that successful blockade of components of the stress response can
result in improved outcome. Hypercoagulability, seen postoperatively in
patients having lower extremity vascular surgery under general anesthesia, is
eliminated when stress ablation is achieved. Unfortunately, stimuli from
upper abdominal and thoracic surgery are difficult to block completely with
regional techniques. In these cases, direct suppression of sympathetic
nervous system by The discovery of opioid receptors in the dorsal column of the spinal cord suggested the addition of a neuraxial opioid to induce analgesia. This practice is now common, and the combination of opioids and local anesthetic agents is used to advantage, especially in the management of postoperative pain. Unattenuated surgical stimuli cause sensitization of excitable spinal neurons, a phenomenon called neuroplasticity (King et al., 1988) or 'wind-up.' This condition produces long-lasting depolarization of posterior horn neurons and heightens the perception of pain. Wind-up can be prevented by intense blockade prior to the stimulus (preemptive analgesia) as with epidural or spinal anesthesia, or by adequately performed local infiltration of the proposed incision site. Complications of regional anesthesia include 'high' spinal blockade, hypotension, headache, cardiac and vascular toxicity, neuropathies, and epidural hematoma. |
Postoperative Period
|
The postoperative period can be a turbulent experience for patients and health-care providers. In addition to the emergence phenomena listed above, other problems arise involving the airway, lungs, and cardiovascular system. Airway obstruction may occur because residual anesthesia effects
continue partially to obtund consciousness and reflexes (especially seen
among patients who normally snore or who have sleep apnea). Strong
inspiratory efforts against a closed glottis can lead to negative-pressure
pulmonary edema. Pulmonary functional residual capacity is reduced
postoperatively following all types of anesthesia and surgery, and hypoxemia
may occur. Hypertension can be prodigious and must be treated with Pain control can be complicated in the immediate postoperative period, especially if opioids have not been part of a balanced anesthetic. Administration of opioids in the recovery room can be problematic among patients who still have a substantial residual anesthetic effect. Patients can alternate between screaming in apparent agony and being deeply somnolent with airway obstruction, all in a matter of moments. The nonsteroidal antiinflammatory agent ketorolac (30 to 60 mg intravenously) frequently is effective, and the development of cyclooxygenase-2 inhibitors (see Chapter 27: Analgesic-Antipyretic and Antiinflammatory Agents and Drugs Employed in the Treatment of Gout) holds promise for analgesia without respiratory depression. Regional anesthetic techniques are an important part of a
perioperative 'multimodal' approach that employs local anesthetic
wound infiltration, epidural, spinal, and plexus blocks, nonsteroidal
antiinflammatory drugs, opioids, Patient-controlled administration of intravenous and epidural analgesics makes use of small computerized pumps activated on demand but programmed with safety limits to prevent overdose. The agents used are opioids (frequently morphine) by the intravenous route and opioid, local anesthetic, or both, by the epidural route. These techniques have revolutionized postoperative pain management, which can be continued for hours or days, promoting ambulation and improved bowel function while oral medications are stabilized. Nausea and Vomiting Nausea and vomiting in the postoperative period continue to be a significant problem following general anesthesia and are caused by an action of anesthetics on the chemoreceptor trigger zone and the brainstem vomiting center, which are modulated by serotonin, histamine, ACh muscarinic, and dopamine receptors. The 5-HT3 serotonin receptor antagonist ondansetron (see Chapter 38: Prokinetic Agents, Antiemetics, and Agents Used in Irritable Bowel Syndrome) is very effective in suppressing nausea and vomiting. Common treatment also includes droperidol, metaclopromide, dexamethasone, and avoidance of N2O. The use of propofol as an induction agent and the nonsteroidal antiinflammatory drug ketorolac as a substitute for opioids may decrease the incidence and severity of postoperative nausea and vomiting. |
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 24094
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2024 . All rights reserved