| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Chemotherapy of Microbial Diseases
Overview
|
Antimicrobial agents, the general classes of these drugs, and their mechanisms of action and mechanisms of bacterial resistance are reviewed in this chapter. The principles that are important for the selection of the appropriate antibiotic, the use of antibiotic combinations, and the role of chemoprophylaxis are discussed. This chapter presents both a philosophical and a practical approach to the appropriate use of antimicrobial agents as well as a discussion of the factors that influence the outcome of such treatment. Also emphasized is the frequent misuse of antimicrobial agents due to lack of identification of the responsible microorganism, leading in some cases to superinfection. |
Antimicrobial Agents: General Considerations: Introduction
|
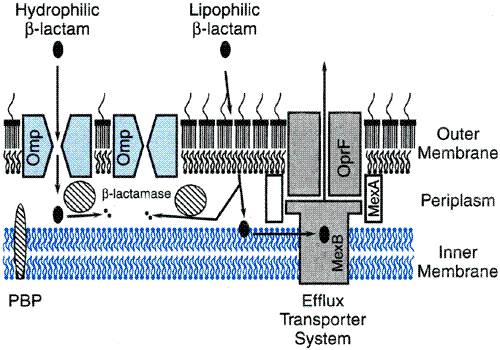
History Pasteur and Joubert were among the first to recognize the potential of microbial products as therapeutic agents. In 1877, they published their observations that common microorganisms could inhibit growth of anthrax bacilli in urine. The modern era of antimicrobial chemotherapy dates to 1936, with the introduction of sulfanilamide into clinical practice. Penicillin became available in quantities sufficient for clinical use in 1941. Streptomycin, chloramphenicol, and chlortetracycline were identified toward the end of or soon after World War II. Since then, numerous classes of antimicrobial agents have been discovered, and literally hundreds of drugs are available for use today. Antimicrobials are among the most commonly used of all drugs. For example, 30% or more of all hospitalized patients are treated with one or more courses of antimicrobial therapy. Death from an incurable bacterial infection came to be considered a thing of the past. However, antimicrobial agents also are among the drugs most commonly misused by physicians. Although antibacterial agents are universally recognized as having no antiviral activity, 50% or more of patients diagnosed with a viral respiratory tract infection are prescribed a course of antibacterial therapy. The inevitable consequence of the widespread use of antimicrobial agents has been the emergence of antibiotic-resistant pathogens, fueling an ever-increasing need for new drugs and contributing to the rising costs of medical care. Moreover, the pace of antimicrobial drug development has dramatically slowed during the last decade, with only a handful of new agents, few of which are really novel, being introduced into clinical practice each year. If the gains in the treatment of infectious diseases are to be preserved, physicians must be wiser and more selective in the use of antimicrobial agents. Definition and Characteristics In the strictest sense, antibiotics are substances produced by various species of microorganisms (bacteria, fungi, actinomycetes) that suppress the growth of other microorganisms. Common usage often extends the term antibiotics to include synthetic antimicrobial agents, such as sulfonamides and quinolones. Hundreds of antibiotics have been identified and developed to the stage where they are of value in the therapy of infectious diseases. Antibiotics differ markedly in physical, chemical, and pharmacological properties, in antibacterial spectra, and in mechanisms of action. Knowledge of molecular mechanisms of bacterial, fungal, and viral replication has greatly facilitated rational development of compounds that can interfere with the life cycles of microorganisms. Classification and Mechanism of Action Several schemes have been proposed to classify and group antimicrobial agents, and all are hampered by exceptions and overlaps. Historically, the most common classification has been based on chemical structure and proposed mechanism of action, as follows: (1) agents that inhibit synthesis of bacterial cell walls; these include the penicillins and cephalosporins, which are structurally similar, and dissimilar agents such as cycloserine, vancomycin, bacitracin, and the azole antifungal agents (e.g., clotrimazole, fluconazole, and itraconazole); (2) agents that act directly on the cell membrane of the microorganism, affecting permeability and leading to leakage of intracellular compounds; these include the detergents such as polymyxin and the polyene antifungal agents nystatin and amphotericin B, which bind to cell-wall sterols; (3) agents that affect the function of 30S or 50S ribosomal subunits to cause a reversible inhibition of protein synthesis; these bacteriostatic drugs include chloramphenicol; the tetracyclines; erythromycin; clindamycin; and pristinamycins; (4) agents that bind to the 30S ribosomal subunit and alter protein synthesis, which eventually leads to cell death; these include the aminoglycosides; (5) agents that affect bacterial nucleic acid metabolism, such as the rifamycins (e.g., rifampin), which inhibit RNA polymerase, and the quinolones, which inhibit topoisomerases; (6) the antimetabolites, including trimethoprim and the sulfonamides, which block essential enzymes of folate metabolism; and (7) antiviral agents, which are of several classes including: (a) nucleic acid analogs, such as acyclovir or ganciclovir, that selectively inhibit viral DNA polymerase, and zidovudine or lamivudine, which inhibit reverse transcriptase; (b) nonnucleoside reverse transcriptase inhibitors, such as nevirapine or efavirenz; and (c) inhibitors of other essential viral enzymes, e.g., inhibitors of HIV protease or influenza neuraminidase. Additional categories likely will emerge as more complex mechanisms are elucidated.The precise mechanism of action of some antimicrobial agents is unknown. Factors That Determine the Susceptibility and Resistance of Microorganisms to Antimicrobial Agents Successful antimicrobial therapy of an infection depends on several factors. In simplest terms, the concentration of antibiotic at the site of infection must be sufficient to inhibit growth of the offending microorganism. If host defenses are intact and active, a minimum inhibitory effect, such as that provided by bacteriostatic agents (i.e., agents that interfere with growth or replication of the microorganism, but do not kill it), may be sufficient. On the other hand, if host defenses are impaired, antibiotic-mediated killing (i.e., a bactericidal effect) may be required to eradicate the infection. Concentration of drug at the site of infection must not only inhibit the organism, but also must remain below the level that is toxic to human cells. If this can be achieved, the microorganism is considered to be susceptible to the antibiotic. If an inhibitory or bactericidal concentration cannot be achieved safely, then the microorganism is considered resistant to that drug. The achievable concentration for an antibiotic in serum typically guides selection of the breakpoint for designating a microorganism as either susceptible or resistant by in vitro susceptibility testing. However, the concentration at the site of infection may be considerably lower than achievable serum concentrations (e.g., vitreous fluid of the eye or cerebrospinal fluid). Local factors (e.g., low pH, high protein concentration) also may impair drug activity. Thus, the drug may be only marginally effective or ineffective in such cases even though standardized in vitro tests would likely report the microorganism as 'sensitive.' Conversely, concentrations of drug in urine may be much higher than those in plasma. Microorganisms reported as 'resistant' may thus respond to therapy when infection is limited to the urinary tract. Bacterial Resistance to Antimicrobial Agents For an antibiotic to be effective, it must reach its target, bind to it, and interfere with its function. Bacterial resistance to an antimicrobial agent falls into three general categories: (1) the drug does not reach its target; (2) the drug is not active; or (3) the target is altered (Davies, 1994; Nikaido, 1994; Spratt, 1994). The outer membrane of gram-negative bacteria is a permeability barrier
that excludes large polar molecules from entering the cell. Small polar
molecules, including many antibiotics, enter the cell through channels made
up of proteins called porins. Absence of, mutation in, or loss of the
appropriate porin channel can slow the rate of drug entry into the cell or
prevent entry altogether, reducing the effective drug concentration at the
target site. If the target is intracellular and the drug requires active
transport across the cell membrane, a mutation or environmental condition
that shuts down this transport mechanism can confer resistance. For example, gentamicin
is actively transported across the cell membrane. Energy for this process is
provided by the electrochemical gradient across the cell membrane. This
gradient is generated by the respiratory enzymes that couple electron
transport and oxidative phosphorylation. A mutation in an enzyme in this
pathway or anaerobic conditions (oxygen is the terminal electron acceptor of
this pathway, and its absence reduces the potential energy across the
membrane) reduces the amount of gentamicin that enters the cell, resulting in
resistance. Bacteria also have efflux pumps that may transport drugs out of
the cell. Resistance to tetracycline and to
Inactivation
of drug is the second general mechanism of drug resistance. Bacterial
resistance to aminoglycosides and to Alteration of the target may be due to mutation of the natural target (fluoroquinolone resistance), target modification (ribosomal protection type of resistance to macrolides and tetracyclines), or substitution with a resistant alternative to the native, susceptible target (methicillin resistance in staphylococci). This mechanism of resistance is due to reduced binding of drug by the critical target or substitution of a new target that does not bind the drug for the native target. Resistance may be acquired by mutation and selection, with passage of the trait vertically to daughter cells. For mutation and selection to be successful in generating resistance, the mutation cannot be lethal and should not appreciably alter virulence. Also, for the trait to spread, the original mutant or its progeny have to be transmitted directly; otherwise, the mutation must be 'rediscovered' by an unrelated mutant within a susceptible strain. More commonly, resistance is acquired by horizontal transfer of
resistance determinants from a donor cell, often of another bacterial
species, by transduction, transformation, or conjugation. Resistance that is
acquired by horizontal transfer can become rapidly and widely disseminated
either by clonal spread of the resistant strain itself or by further genetic
transfers from the resistant strain to other susceptible strains. The
staphylococcal Mutations Mutation and antibiotic selection of the resistant mutant are the molecular basis for resistance to streptomycin (ribosomal mutation), quinolones (gyrase gene mutation), and rifampin (RNA polymerase gene mutation). This mechanism underlies the drug resistance of M. tuberculosis to antituberculous agents. Mutations may occur in the gene encoding (1) the target protein, altering its structure so that it no longer binds the drug; (2) a protein involved in drug transport; (3) a protein important for drug activation; or (4) in a regulatory gene or promoter affecting expression of the target, a transport protein, or an inactivating enzyme. Any large population of antibiotic-susceptible bacteria is likely to contain some mutants that are relatively resistant to the drug. Mutations are not the result of exposure to the particular drug; rather, they are random events that confer a survival advantage upon reexposure to the drug. In some instances a single-step mutation results in a high degree of resistance. For example, a point mutation within the drug-binding domain in the beta subunit of bacterial RNA polymerase confers high-level resistance to rifampin. In other cases the emergence of resistant mutants may require several steps, each step conferring only slight alterations in susceptibility. High-level resistance of E. coli. to fluoroquinolones is due to accumulation of multiple stepwise mutations. Transduction Transduction is acquisition of bacterial DNA from a bacteriophage (a virus that propagates on bacteria) that has incorporated DNA from a previous host bacterium within its outer protein coat. If the DNA includes a gene for drug resistance, a newly infected bacterial cell may become resistant to the agent and capable of passing the trait on to its progeny. Transduction is particularly important in the transfer of antibiotic resistance among strains of Staphylococcus aureus, where some phages can carry plasmids (autonomously replicating pieces of extrachromosomal DNA) that code for penicillinase, while others transfer genes encoding resistance to erythromycin, tetracycline, or chloramphenicol. Transformation This method of transferring genetic information involves uptake and incorporation of DNA that is free in the environment into the host genome by homologous recombination. Transformation is the molecular basis of penicillin resistance in pneumococci and Neisseria (Spratt, 1994). Penicillin-resistant pneumococci produce altered penicillin-binding proteins (PBPs) that have low-affinity binding of penicillin. Nucleotide sequence analysis of the genes encoding these altered PBPs indicates that they are mosaics in which blocks of foreign DNA from a closely related species of streptococcus have been imported and incorporated into the resident PBP gene. Conjugation The passage of genes from cell to cell by direct contact through a sex
pilus or bridge is termed conjugation. This is an extremely important
mechanism for spread of antibiotic resistance, since DNA that codes for
resistance to multiple drugs may be so transferred. The clinical importance of
conjugation was first recognized in Genetic transfer by conjugation is common among gram-negative bacilli, and resistance is conferred on a susceptible cell as a single event. Enterococci also contain broad host-range conjugative plasmids which are involved in the transfer and spread of resistance genes among gram-positive organisms. Vancomycin resistance in enterococci is mediated by a conjugative plasmid (Arthur and Courvalin, 1993; Murray, 2000). Conjugation with genetic exchange between nonpathogenic and pathogenic microorganisms probably occurs in the intestinal tract of human beings and in animals. The efficiency of transfer is low; however, antibiotics can exert a powerful selective pressure to allow emergence of the resistant strain. The proportion of enteric bacteria that carry plasmids for multiple-drug resistance has thus risen inexorably in the past 30 years. In some studies, more than 50% of persons have been found to carry multiply resistant coliform bacilli. Such bacteria have been isolated in large numbers from rivers containing untreated sewage and from animals. Multiply resistant Enterobacteriaceae have become a problem worldwide, creating an insatiable need for new antibiotics. In several situations where antibiotic usage has been controlled, the rate of emergence of these resistant strains was slowed; in some instances their incidence was actually reduced. The recent emergence of antibiotic resistance in bacterial pathogens,
both nosocomially and in the community setting, is a very serious development
that threatens the end of the antibiotic era. Penicillin-resistant strains of
pneumococci account for 50% or more of isolates in some European countries,
and the proportion of such strains is rising in the |
Selection of an Antimicrobial Agent
|
Optimal and judicious selection of antimicrobial agents for the therapy of infectious diseases requires clinical judgment and detailed knowledge of pharmacological and microbiological factors. Unfortunately, the decision to use antibiotics frequently is made lightly, without regard to the potential infecting microorganism or to the pharmacological features of the drug. Antibiotics are used in three general waysas empirical therapy, as definitive therapy, and as prophylactic or preventive therapy. When used as empirical, or initial, therapy, the antibiotic must 'cover' all of the likely pathogens, since the infecting organism(s) has not yet been defined. Combination therapy or treatment with a single broad-spectrum agent often is employed. However, once the infecting microorganism is identified, definitive antimicrobial therapy should be instituteda narrow-spectrum, low-toxicity regimen to complete the course of treatment. When an antimicrobial agent is indicated, the goal is to choose a drug that is selectively active for the most likely infecting microorganism(s) and that has the least potential to cause toxicity or allergic reactions in the individual being treated (see Table 431). The first decision to be made is whether or not administration of an antimicrobial agent is even indicated. The reflex action of many physicians is to associate fever with treatable infections and prescribe antimicrobial therapy without further evaluation. This practice is irrational and potentially dangerous. The diagnosis may be masked if appropriate cultures are not obtained prior to therapy. Antibiotics can cause serious toxicity, and injudicious use of antimicrobial agents promotes selection of resistant microorganisms. Of course, definitive identification of a bacterial infection before treatment is initiated often is not possible. In the absence of a clear indication, antibiotics often may be used if disease is severe and if it seems likely that withholding therapy will result in failure to manage a potentially life-threatening infection. Initiation of optimal empirical antibiotic therapy requires a knowledge of the most likely infecting microorganisms and their susceptibilities to antimicrobial drugs. A number of techniques are helpful in the selection of an antibiotic regimen. The clinical picture may suggest the specific microorganism. Knowledge of the microorganisms most likely to cause specific infections in a given host is essential. In addition, simple and rapid laboratory techniques are available for the examination of infected tissues. The most valuable and time-tested method for immediate identification of bacteria is the examination of the infected secretion or body fluid with Gram's stain. Tests such as this one help to narrow the list of potential pathogens and permit more rational selection of initial antibiotic therapy. However, in most situations, identification of the morphology of the infecting organism is not adequate to arrive at a specific bacteriological diagnosis, and the selection of a single narrow-spectrum antibiotic may be inappropriate, particularly if the infection is life-threatening. Broad antimicrobial coverage is then indicated, pending isolation and identification of the microorganism. Whenever the clinician is faced with initiating therapy on a presumptive bacteriological diagnosis, cultures of the presumed site of infection and blood, if bacteremia is a possibility, should be taken prior to the institution of drug therapy. For definitive therapy, the regimen should be changed to a more specific (narrow-spectrum) antimicrobial agent once an organism has been isolated and results of susceptibility tests are known. Testing for Microbial Sensitivity to Antimicrobial Agents There may be wide variations in the susceptibility of different strains of the same bacterial species to antibiotics. Information about the pattern of sensitivity of the infecting microorganism is important for appropriate drug selection. Several tests are now available for determination of bacterial sensitivity to antimicrobial agents. The most commonly used are disk-diffusion, agar- or broth-dilution tests, and automated test systems. The disk-diffusion technique provides only qualitative or semiquantitative information on the susceptibility of a given microorganism to a given antibiotic. The test is performed by applying commercially available filter-paper disks impregnated with a specific amount of the drug onto an agar surface, over which a culture of the microorganism has been streaked. After 18 to 24 hours of incubation, the size of a clear zone of inhibition around the disk is measured. The diameter of the zone depends upon the activity of the drug against the test strain. Standardized values for zone sizes for each bacterial species and each antibiotic permit classification of the clinical isolate as resistant, intermediate, or susceptible. Dilution tests employ antibiotics in serially diluted concentrations in solid agar or broth media containing a culture of the test microorganism. The lowest concentration of the agent that prevents visible growth after 18 to 24 hours of incubation is known as the minimal inhibitory concentration (MIC), and the lowest concentration that results in a 99.9% decline in bacterial numbers is known as the minimal bactericidal concentration (MBC). The value of the MBC as a clinical test has not been established. Automated systems also use a broth-dilution method. The optical density of a broth culture of the clinical isolate incubated in the presence of drug is measured by absorbance densitometry. If the density of the culture exceeds a threshold optical density, then growth has occurred at that concentration of drug. The MIC is the concentration at which the optical density remains below the threshold. Pharmacokinetic Factors In vitro activity, although critical, is only a guide as to whether or not an antibiotic is likely to be effective in an infection. Successful therapy also depends upon achieving a drug concentration that is sufficient to inhibit or kill bacteria at the site of the infection without harming the host. To accomplish this therapeutic goal, several pharmacokinetic and host factors must be evaluated. The location of the infection may, to a large extent, dictate the choice of drug and the route of administration. The minimal drug concentration achieved at the infected site should be approximately equal to the MIC for the infecting organism, although in most instances it is advisable to achieve multiples of this concentration if possible. However, there is evidence to suggest that even subinhibitory concentrations of antibiotics may enhance phagocytosis (Nosanchuk et al., 1999) and may be effective. Although these and related observations may explain why some infections are cured even when inhibitory concentrations are not achieved, it should be the aim of antimicrobial therapy to produce antibacterial concentrations of drug at the site of infection during the dosing interval. This can be achieved only if the pharmacokinetic and pharmacodynamic principles presented in Chapters 1: Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, and Elimination and 2: Pharmacodynamics: Mechanisms of Drug Action and the Relationship Between Drug Concentration and Effect are understood and employed. Access of antibiotics to sites of infection depends on multiple factors. If the infection is in the cerebrospinal fluid (CSF), the drug must pass the blood-brain barrier, and many antimicrobial agents that are polar at physiological pH do so poorly; some, such as penicillin G, are actively transported out of the CSF by an anion transport mechanism in the choroid plexus. The concentrations of penicillins and cephalosporins in the CSF are usually only 0.5% to 5% of steady-state concentrations determined simultaneously in plasma. However, the integrity of the blood-brain barrier is diminished during active bacterial infection; tight junctions in cerebral capillaries open, leading to a marked increase in the penetration of even polar drugs (Quagliarello and Scheld, 1997). As the infection is eradicated and the inflammatory reaction subsides, penetration reverts toward normal. Since this may occur while viable microorganisms persist in the CSF, drug dosage should not be reduced as the patient improves until the CSF is presumed or proven to be sterile. Penetration of drugs into infected loci almost always depends on passive diffusion. The rate of penetration is thus proportional to the concentration of free drug in the plasma or extracellular fluid. Drugs that are extensively bound to protein thus may not penetrate to the same extent as those that are bound to a lesser extent. Drugs that are highly protein bound also may have reduced activity, because only the unbound fraction of drug is free to interact with its target. Traditionally, the dose and dosing frequency of antibiotics have been
selected to achieve antibacterial activity at the site of infection for most
of the dosing interval. However, controversy exists as to whether the
therapeutic effect achieved from relatively constant antibacterial activity
is superior to that from high peak concentrations followed by periods of
subinhibitory activity. To a certain extent, this depends upon whether a drug
exhibits concentration-dependent or time-dependent growth inhibition (Craig,
1998). The activity of Knowledge of the status of the individual patient's mechanisms for elimination of drugs also is essential, especially when excessive plasma or tissue concentrations of the drugs may cause serious toxicity. Most antimicrobial agents and their metabolites are eliminated primarily by the kidneys. Specific nomograms are available to facilitate adjustment of dosage of many such agents in patients with renal insufficiency. These are discussed in the chapters dealing with the individual drugs and in Appendix II. One must be particularly careful when using aminoglycosides, vancomycin, or flucytosine in patients with impaired renal function, since these drugs are eliminated exclusively by renal mechanisms, and their toxicity appears to correlate with their concentration in plasma and tissue. If renal toxicity of a drug that is cleared by the kidney occurs and care is not exercised, a vicious cycle may ensue. For drugs that are metabolized or excreted by the liver (erythromycin, chloramphenicol, metronidazole, clindamycin), dosages may have to be reduced in patients with hepatic failure. Route of Administration The discussion of choice of routes of administration that appears in Chapter 1: Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, and Elimination of course applies to antimicrobial agents. While oral administration is preferred whenever possible, parenteral administration of antibiotics usually is recommended in seriously ill patients in whom predictable concentrations of drug must be achieved. Specific factors that govern the choice of route of administration for individual agents are discussed in the chapters that follow. Host Factors Innate host factors can be the prime determinants not only of the type of drug selected but also of its dosage, route of administration, risk and nature of untoward effects, and therapeutic effectiveness. Host Defense Mechanisms A critical determinant of the therapeutic effectiveness of antimicrobial agents is the functional state of host defense mechanisms. Both humoral and cellular immunity are important. Inadequacy of type, quality, and quantity of the immunoglobulins; alteration of the cellular immune system; or a qualitative or quantitative defect in phagocytic cells may result in therapeutic failure despite the use of otherwise appropriate and effective drugs. Frequently, infection in the immunocompetent host can be cured merely by halting multiplication of the microorganisms (a bacteriostatic effect). If host defenses are impaired, bacteriostatic activity may be inadequate and a bactericidal agent may be required for cure. Examples include bacterial endocarditis, where phagocytic cells are absent from the infected site; bacterial meningitis, where phagocytic cells are ineffective because of lack of opsonins; and disseminated bacterial infections in neutropenic patients, where the total mass of phagocytic cells is reduced. Patients with acquired immunodeficiency syndrome (AIDS) have impaired cellular immune responses, and therapy for various opportunistic infections in these patients is often suppressive but not curative. For example, most AIDS patients with bacteremia due to Salmonella will respond to conventional therapy, but this infection will relapse even after prolonged treatment (Jacobson et al., 1989), and treatment of disseminated atypical mycobacterial infection is lifelong. Local Factors Cure of an infection with antibiotics depends on an understanding of how local factors at the site of infection affect the antimicrobial activity of the drug. Antimicrobial activity may be significantly reduced in pus, which contains phagocytes, cellular debris, and proteins that can bind drugs or create conditions unfavorable to drug action (Bamberger et al., 1993; Konig et al., 1998). Large accumulations of hemoglobin in infected hematomas can bind penicillins and tetracyclines and may thus reduce the effectiveness of the drugs (Craig and Kunin, 1976). The pH in abscess cavities and in other confined infected sites (pleural space, CSF, and urine) is usually low, resulting in a marked loss of antimicrobial activity of aminoglycosides, erythromycin, and clindamycin (Strausbaugh and Sande, 1978). However, some drugs, such as chlortetracycline, nitrofurantoin, and methenamine, are more active in such an acidic environment. The anaerobic conditions found in abscess cavities impair activity of the aminoglycosides (Verklin and Mandell, 1977). Penetration of antimicrobial agents into infected areas such as abscess cavities is impaired, because the vascular supply is reduced. Successful therapy of abscesses usually requires drainage. The presence of a foreign body in an infected site markedly reduces the likelihood of successful antimicrobial therapy. Prosthetic material [e.g., prosthetic cardiac valves, prosthetic joints, pacemakers, vascular grafts, and various vascular and central nervous system (CNS) shunts] is perceived by phagocytic cells as foreign. In an attempt to phagocytose and destroy it, degranulation occurs, resulting in the depletion of intracellular bactericidal substances. Thus, these phagocytes are relatively inefficient in killing bacterial pathogens. Bacteria also may reside within phagocytes, sequestered from most antimicrobial agents (Zimmerli et al., 1984). There also is evidence that bacteria adhering to prosthetic material resist killing by bactericidal agents (Chuard et al., 1991). Infections associated with foreign bodies are thus characterized by frequent relapses and failure, even with long-term, high-dose antibiotic therapy. Successful therapy usually requires removal of the foreign material. Infectious agents that reside within phagocytic cells (intracellular parasites) are protected from the action of many antimicrobial agents that penetrate into cells poorly. This may be a problem in infections with Salmonella, Brucella, Toxoplasma, Listeria, and M. tuberculosis and, in some instances, even in infections caused by S. aureus. Certain antibioticsfor example, fluoroquinolones, isoniazid, trimethoprim-sulfamethoxazole, and rifampinpenetrate cells well and can achieve intracellular concentrations that inhibit or kill pathogens residing within cells. Age The age of the patient is an important determinant of pharmacokinetic properties of antimicrobial agents (see Chapter 1: Pharmacokinetics: The Dynamics of Drug Absorption, Distribution, and Elimination). Mechanisms of elimination, especially renal excretion and hepatic biotransformation, are poorly developed in the newborn, especially the premature infant. Failure to make adjustments for such differences can have disastrous consequences (e.g., see discussion of the 'gray-baby syndrome,' caused by chloramphenicol, in Chapter 47: Antimicrobial Agents: Protein Synthesis Inhibitors and Miscellaneous Antibacterial Agents). Elderly patients may clear renally eliminated drugs less well because of reduced creatinine clearance. They also may metabolize drugs less rapidly, predisposing them to elevated and potentially toxic concentrations of drugs when compared to younger patients. Elderly patients often are more likely to suffer toxicity at otherwise safe concentrations of drugs, as is the case for aminoglycoside ototoxicity. Developmental factors also may determine the type of untoward response to a drug. Tetracyclines bind avidly to developing teeth and bones, and their use in young children can result in retardation of bone growth and discoloration or hypoplasia of tooth enamel. Fluoroquinolones accumulate in cartilage of developing bone, affecting its growth. Kernicterus may follow the use of sulfonamides in newborn infants, because this class of drugs competes effectively with bilirubin for binding sites on plasma albumin. Achlorhydria in young children and in the elderly or antacid therapy may alter absorption of orally administered antimicrobial agents (e.g., increased absorption of penicillin G and decreased absorption of ketoconazole). Genetic Factors Certain genetic or metabolic abnormalities must be considered when prescribing antibiotics. A number of drugs (e.g., sulfonamides, nitrofurantoin, chloramphenicol, and nalidixic acid) may produce acute hemolysis in patients with glucose-6-phosphate dehydrogenase deficiency. Patients who acetylate isoniazid rapidly may have subtherapeutic concentrations of the drug in plasma. Pregnancy Pregnancy may impose an increased risk of reaction to antimicrobial agents for both mother and fetus. Hearing loss in the child has been associated with administration of streptomycin to the mother during pregnancy. Tetracyclines can affect the bones and teeth of the fetus. Pregnant women receiving tetracycline may develop fatal acute fatty necrosis of the liver, pancreatitis, and associated renal damage. Pregnancy also may affect the pharmacokinetics of various antibiotics. The lactating female can pass antimicrobial agents to her nursing child. Both nalidixic acid and sulfonamides in breast milk have been associated with hemolysis in children with glucose-6-phosphate dehydrogenase deficiency. In addition, sulfonamides, even in the small amounts received from breast milk, may predispose the nursing child to kernicterus (Vorherr, 1974). Drug Allergy Antibiotics, especially Disorders of the Nervous System Patients predisposed to seizures are at risk for localized or major
motor seizures while taking high doses of penicillin G. This neurotoxicity of
penicillin and other |
Therapy with Combined Antimicrobial Agents
|
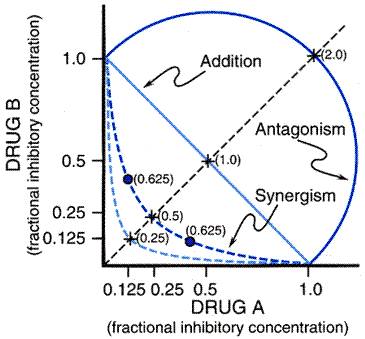
The simultaneous use of two or more antimicrobial agents has a certain rationale and is recommended in specifically defined situations (Table 431). However, selection of an appropriate combination requires an understanding of the potential for interaction between the antimicrobial agents. Interactions may affect either the microorganism or the patient. Antimicrobial agents acting at different targets may enhance or impair overall antimicrobial activity. A combination of drugs may have additive or superadditive toxicities in the patient. For example, vancomycin given alone usually has minimal nephrotoxicity. However, when vancomycin is given with an aminoglycoside, the toxicity of the aminoglycoside is increased (Farber and Moellering, 1983). Methods of Testing Antimicrobial Activity of Drug Combinations Two methods are used to measure antimicrobial activity of drug combinations. The first employs serial twofold dilutions of antibiotics in broth inoculated with a standard number of the test microorganism in a checkerboard array, so that a large number of antibiotic concentrations in different proportions can be tested simultaneously (Figure 432). The concentrations of each drug, singly and in combination, that prevent visible growth are determined after an 18- to 24-hour incubation. Synergism is defined as inhibition of growth by a combination of drugs at concentrations less than or equal to 25% of the MIC of each drug acting alone. This implies that one drug is affecting the microorganism in such a way that it becomes more sensitive to the inhibitory effect of the other. If one-half of the inhibitory concentration of each drug is required to produce inhibition, the result is called additive [fractional inhibitory concentration (FIC) index = 1; see Figure 432], suggesting that the two drugs are working independently of each other. If more than one-half of the MIC of each drug is necessary to produce the inhibitory effect, the drugs are said to be antagonistic (FIC index >1). When the drugs are tested for a variety of proportionate drug concentrations, as with the checkerboard technique, an isobologram may be constructed (Figure 432). Synergism is shown by a concave curve, the additive effect by a straight line, and antagonism by a convex curve. A potential limitation of this method is that its endpoint is growth inhibition, not killing. Consequently, synergism may not indicate enhanced bactericidal effect.
The second method for evaluating drug combinations is the time-kill curve, which assays bactericidal activity. Identical cultures are incubated simultaneously with antibiotics added singly or in combination. Quantitative subcultures are taken over time to determine the number of bacteria remaining. If a combination of antibiotics is more bactericidal than either drug alone, typically defined as at least a 100-fold reduction in the inoculum for the combination compared to the most active single agent, the result is termed synergism. If the combination kills fewer bacteria than the most active drug alone, antagonism is said to occur. If the combination kills the same number of bacteria or results in less than a 100-fold reduction in the inoculum compared to the most active single drug, the result is called indifference. Jawetz and Indications for the Clinical Use of Combinations of Antimicrobial Agents Use of a combination of antimicrobial agents may be justified (1) for empirical therapy of an infection in which the cause is unknown; (2) for treatment of polymicrobial infections; (3) to enhance antimicrobial activity (i.e., synergism) for a specific infection; or (4) to prevent emergence of resistance. Empirical Therapy of Severe Infections in Which a Cause Is Unknown Empirical therapy of infections is probably the most common reason for using a combination of antibiotics. Knowledge of the type(s) of infection, its microbiology, and the spectrum of activity of the several potentially useful antimicrobial agents is essential for selection of a rational and effective regimen. Severe illness and less certainty as to the particular infection or the causative agent may mandate broad coverage initially. More than one agent may be required to ensure that the regimen includes an agent that is active against the potential pathogens (for example, in the treatment of community-acquired pneumonia, a macrolide for atypical organisms such as mycoplasma and cefuroxime for gramnegative pathogens). Prolonged administration of empirical, broad-spectrum coverage or multiple antibiotics, however, should be avoided. It is often unnecessary (e.g., the infection is caused by a single pathogen or no infection is documented) and unnecessarily expensive. Moreover, toxicity, superinfection, and selection of multiple-drug-resistant microorganisms may result. Inappropriately broad coverage often arises because the physician fails to obtain adequate cultures prior to the initiation of therapy or fails to discontinue the combination chemotherapy after the microorganism has been identified and its antimicrobial susceptibilities are known. Although reluctance to change antimicrobial agents is understandable when a favorable clinical response has occurred, the goal should be to use the most selectively active drug that produces the fewest adverse effects. Treatment of Polymicrobial Infections Treatment of intraabdominal, hepatic, and brain abscesses and some genital tract infections may require the use of a drug combination to eradicate these typically mixed aerobic-anaerobic infections. These and other mixed infections may be caused by two or more microorganisms that are sufficiently different in antimicrobial susceptibility such that no single agent can provide the required coverage. Enhancement of Antibacterial Activity in the Treatment of Specific Infections Antimicrobial agents administered together may produce a synergistic effect. Synergistic combinations of antimicrobial agents have been shown to be better than single-agent therapy in relatively few infections. Perhaps the best-documented example of the utility of a synergistic combination of antimicrobial agents is in the treatment of enterococcal endocarditis (Wilson et al., 1995). In vitro, penicillin alone is bacteriostatic against strains of E. faecalis or E. faecium, whereas a combination of penicillin and streptomycin or gentamicin is bactericidal. Treatment of enterococcal endocarditis with penicillin alone frequently results in relapses, whereas combination therapy is curative. Penicillin and streptomycin or gentamicin also are synergistic in vitro against strains of viridans streptococci. This combination eradicates bacteria from infected valvular vegetations more rapidly than does penicillin alone in animal models. A two-week course of treatment with the combination is just as effective as a four-week penicillin-only regimen for patients with streptococcal endocarditis. Synergism in vitro and in experimental models in vivo by a combination of a penicillin and an aminoglycoside also has been demonstrated with S. aureus. Selected patients with tricuspid valve endocarditis caused by S. aureus can be treated successfully with nafcillin and a low dose of tobramycin or gentamicin administered for a total of 2 weeks, instead of the 4 to 6 weeks of nafcillin alone traditionally used to treat this disease (Chambers et al., 1988).
The combination of a sulfonamide and an inhibitor of dihydrofolate reductase, such as trimethoprim, is synergistic due to the blocking of sequential steps in microbial folate synthesis. A fixed combination of sulfamethoxazole and trimethoprim, which is active against organisms that may be resistant to sulfonamides alone, is effective for treatment of urinary tract infections, Pneumocystis carinii pneumonia, typhoid fever, shigellosis, and certain infections due to ampicillin-resistant Haemophilus influenzae. The combination of flucytosine and amphotericin B is synergistic against Cryptococcus neoformans in vitro and in animal models of infection. The combination permits lowering the dose of amphotericin B and a 6-week rather than a 10-week duration of therapy with similar cure rates and less toxicity in non-HIV-infected patients with cryptococcal meningitis (Bennett et al., 1979). This combination also has been shown to sterilize the CSF more rapidly than amphotericin B alone in AIDS patients with cryptococcal meningitis (van der Horst et al., 1997). Prevention of the Emergence of Resistant Microorganisms A combination of antibiotics may prevent selection of mutants that are resistant to a single drug. For example, if the frequency of mutation for the acquisition of resistance to one drug is 107 and that for a second drug is 106, the probability of two simultaneous, independent mutations in a single cell is the product of the two frequencies, 1013. The number of organisms that would have to be present for such a mutant to occur is several orders of magnitude greater than that likely to be encountered clinically. This is the theoretical basis for combination chemotherapy of tuberculosis, for which a single agent is likely to fail because of emergence of resistant mutants during therapy. The concomitant use of two or more active agents vastly improves cure rates by preventing development of resistance. Other examples include infections that are treated with rifampin, such as staphylococcal osteomyelitis or prosthetic valve endocarditis (Zimmerli et al., 1998), in which a second agent is added to prevent emergence of rifampin-resistant mutants, and combination therapy of Helicobacter pylori infection (Taylor et al., 1997). Other than for these specific examples, few data document that drug combinations improve outcome by preventing emergence of resistance. Disadvantages of Combinations of Antimicrobial Agents Antimicrobial combinations also can be disadvantageous due to the risk of toxicity from two or more agents, the selection of multiple-drug-resistant microorganisms, and the increased cost to the patient. In addition, as noted above, antagonism of antibacterial effect may result when bacteriostatic and bactericidal agents are given concurrently. The clinical significance of antibiotic antagonism is not well defined. Although antagonism of one antibiotic by another has been a frequent observation in vitro, well-documented clinical examples of this phenomenon are relatively rare. The most notable of these involves the therapy of pneumococcal meningitis. In 1951, Lepper and Dowling reported that the fatality rate among patients with pneumococcal meningitis who were treated with penicillin alone was 21%, while patients who received the combination of penicillin and chlortetracycline had a fatality rate of 79%. This conclusion was supported by Mathies and colleagues (1967), who reported that children with bacterial meningitis of multiple causes treated with ampicillin alone had a 4.3% mortality rate compared to a 10.5% mortality rate in children treated with the combination of ampicillin, chloramphenicol, and streptomycin. Antagonism between antibiotics is probably relatively unimportant in most infections. For antagonism between two antibiotics to occur, both agents must be active against the infecting microorganism. Because the addition of a bacteriostatic drug to a bactericidal drug frequently results in a bacteriostatic effect, in many infections where host defenses are adequate, this is of no consequence. On the other hand, if achieving a bactericidal effect is critical for cure of the infection (e.g., meningitis, endocarditis, and gram-negative infections in neutropenic patients), antagonism of this activity could adversely affect outcome. |
The Prophylaxis of Infection with Antimicrobial Agents
|
A large percentage (from 30% to 50%) of
antimicrobial agents administered in the Chemoprophylaxis is highly effective in some clinical settings, and in others is totally without value and may be deleterious. Use of antimicrobial compounds to prevent infections remains controversial in numerous situations. In general, if a single, effective, nontoxic drug is used to prevent infection by a specific microorganism or to eradicate an early infection, then chemoprophylaxis frequently is successful. On the other hand, if the aim of prophylaxis is to prevent colonization or infection by any or all microorganisms present in the environment of a patient, then prophylaxis often fails. Prophylaxis may be used to protect healthy persons from acquisition of or invasion by specific microorganisms to which they are exposed. Successful examples of this practice include the following: use of rifampin to prevent meningococcal meningitis in people who are in close contact with a case; prevention of gonorrhea or syphilis after contact with an infected person; the intermittent use of trimethoprim-sulfamethoxazole to prevent recurrent urinary tract infections usually caused by E. coli. Antimicrobial prophylaxis is used to prevent a variety of infections in patients undergoing organ transplantation or receiving cancer chemotherapy. Although specific infections often can be prevented, superinfections with opportunistic fungal pathogens or multiple-drug-resistant bacteria can be a problem. Moreover, the infection rate may be apparently lowered without changing overall outcomes. Chemoprophylaxis is recommended for patients with valvular or other structural lesions of the heart predisposing to endocarditis who are undergoing dental, surgical, or other procedures that produce a high incidence of bacteremia (Dajani et al., 1997). Recent data suggesting that dental procedures have a minimal, if indeed any, role in causing endocarditis (Strom et al., 1998) have called some of the recommendations for chemoprophylaxis into question, but the recommendations nevertheless remain the standard of care. A procedure that injures a mucous membrane where there are large numbers of bacteria (such as in the oropharyngeal or gastrointestinal tract) will produce transient bacteremia. Streptococci from the mouth, enterococci from the gastrointestinal or genitourinary tract, and staphylococci from the skin commonly enter the bloodstream and may adhere to an abnormal or damaged valve surface, producing endocarditis. Chemoprophylaxis is directed against these microorganisms. Therapy, generally as a single dose, should not begin until immediately before the procedure, because prolonged administration of antibiotics can lead to colonization by resistant strains. Criteria have been established for the selection of specific drugs and patients who should receive chemoprophylaxis for various procedures. The most extensive and probably best studied use of chemoprophylaxis is to prevent wound infections after various surgical procedures (see Table 432; see Antimicrobial prophylaxis in surgery, 1997). Wound infection results when a critical number of bacteria are present in the wound at the time of closure. Several factors determine the size of this critical inoculum, including virulence of the bacteria, the presence of devitalized or poorly vascularized tissue, the presence of a foreign body, and the status of the host. Antimicrobial agents directed against the invading microorganisms may reduce the number of viable bacteria below the critical level and thus prevent infection. Several factors are important for the effective and judicious use of antibiotics for surgical prophylaxis. First, antimicrobial activity must be present at the wound site at the time of its closure. Thus, the drug should be given immediately preoperatively and perhaps intraoperatively for prolonged procedures. Second, the antibiotic must be active against the most likely contaminating microorganisms. Thus, cephalosporins are commonly used in this form of chemoprophylaxis. Third, there is mounting evidence that the continued use of drugs after the surgical procedure is unwarranted and potentially harmful. No data suggest that the incidence of wound infections is lower if antimicrobial treatment is continued after the day of surgery (Rowlands et al., 1982). Use beyond 24 hours not only is unnecessary, but also leads to the development of more resistant flora and superinfections caused by antibiotic-resistant strains. The risk of toxicity and the unnecessary expense are, of course, additional disadvantages. Chemoprophylaxis should be limited to operative procedures for which there are data supporting its use. A number of studies indicate that it can be justified in dirty and contaminated surgical procedures (e.g., resection of the colon), where the incidence of wound infections is high. These include less than 10% of all surgical procedures. In clean surgical procedures, which account for approximately 75% of the total, the expected incidence of wound infection is less than 5%, and antibiotics should not be used routinely. Exceptions are rational when the surgery involves insertion of a prosthetic implant (e.g., prosthetic valve, vascular graft, prosthetic joint), cardiac surgery, or neurosurgical procedures; the complications of infection are so drastic that most authorities currently agree to chemoprophylaxis with these indications. Of course, the use of systemic antibiotics for chemoprophylaxis during surgical procedures does not reduce the need for sterile and skilled surgical technique. |
Superinfections
|
All individuals who receive therapeutic doses of antibiotics undergo alterations in the normal microbial population of the intestinal, upper respiratory, and genitourinary tracts; some develop superinfection as a result of such changes. Superinfection may be defined as the appearance of bacteriological and clinical evidence of a new infection during the chemotherapy of a primary one. This phenomenon is relatively common and potentially very dangerous because the microorganisms responsible for the new infection are, in many cases, Enterobacteriaceae, Pseudomonas, and Candida or other fungi. These may be very difficult to eradicate with the currently available antiinfective drugs. Superinfection by these microorganisms is due to removal of the inhibitory influence of the normal flora. Normal flora may themselves produce antibacterial substances, and they also presumably compete for essential nutrients. The more 'broad' the effect of an antibiotic on microorganisms, the greater the alteration in the normal microflora and the greater the possibility that a single microorganism will become predominant, invade the host, and produce infection. Thus, the incidence of superinfection is lowest with penicillin G, higher with tetracyclines and chloramphenicol, and highest with combinations of broad-spectrum antimicrobials and the expanded-spectrum third-generation cephalosporins. It can be expected that further development and use of broad-spectrum agents will lead to more extensive alterations in the normal flora and, thus, to more superinfections. The development of agents that kill pathogens selectively while carefully preserving the normal flora would be beneficial. The most specific antimicrobial agent to treat a given infection should be chosen whenever possible. The incidence of superinfection also increases when administration of antibiotics is prolonged. The fact that harmful effects may follow the therapeutic or prophylactic use of antiinfective agents should not discourage the physician from their administration in any situation in which they are definitely indicated. However, the physician should be hesitant to use antimicrobial drugs in instances where evidence of infection is entirely lacking or, at most, only suggestive. To do otherwise is to run the risk, at times, of converting a simple, benign, and self-limited disease into one that may be serious or even fatal. |
Misuses of Antibiotics
|
The purpose of this introductory chapter has been to lay the groundwork for the maximally effective utilization of antimicrobial drugs. A brief discussion of the misuse and overuse of antimicrobial agents is in order. Treatment of Untreatable Infections A common misuse of these agents is in infections that have been proved by experimental and clinical observation to be untreatable: i.e., they do not respond to treatment with antimicrobial agents (Nyquist et al., 1998). The majority of the diseases caused by viruses are self-limited and do not respond to any of the currently available antiinfective compounds. Thus, antimicrobial therapy of measles, mumps, and at least 90% of infections of the upper respiratory tract and many gastrointestinal infections is ineffective and, therefore, useless. Therapy of Fever of Unknown Origin Fever of undetermined cause may be of two types: one that is present for only a few days to a week and another that persists for an extended period. Both of these are frequently (and inappropriately) treated with empirical antimicrobial agents. Fever of short duration, in the absence of localizing signs, is probably associated with undefined viral infections. Antimicrobial therapy is unnecessary and defervescence takes place spontaneously within a week or less. Fever persisting for two or more weeks, commonly referred to as 'fever of unknown origin,' has a variety of causes, of which only about one-quarter are infections (de Kleijn et al., 1997). Some of these infectionsfor example, tuberculosis or disseminated fungal infectionsmay require treatment with antimicrobial agents that are not used for common bacterial infections. Others, such as occult abscesses, may require surgical drainage or prolonged courses of pathogen-specific therapy, as in the case of bacterial endocarditis. Inappropriately administered antimicrobial therapy may serve to mask an underlying infection and contribute to delay in diagnosis, and prevent establishing a microbial etiology by rendering cultures negative. The noninfectious causesincluding regional enteritis, lymphoma, renal cell carcinoma, hepatitis, collagen-vascular disorders, and drug fever, to name a fewdo not respond to antimicrobial agents at all. Rather than embarking on a course of empirical antimicrobial therapy for fever of unknown origin, the physician should search for its cause. Improper Dosage Dosing errors, which can be the wrong frequency of administration or the use of either an excessive or a subtherapeutic dose, are common. Although antimicrobial drugs are among the safest and least toxic of drugs used in medical practice, excessive amounts can result in significant toxicities, including seizures (e.g., penicillin), vestibular damage (aminoglycosides), and renal failure (aminoglycosides), especially in patients with impaired drug excretion or metabolism. The use of too low a dose may result in treatment failure and is most likely to select for microbial resistance. Inappropriate Reliance on Chemotherapy Alone Infections complicated by abscess formation, the presence of necrotic tissue, or the presence of a foreign body often cannot be cured by antimicrobial therapy alone. Drainage, debridement, and removal of the foreign body are just as important as the choice of antimicrobial agent and in some cases more important. Two of many possible examples follow. The patient with pneumonia and empyema often fails to be cured even with administration of large doses of an effective drug unless the infected pleural fluid is drained. The patient with S. aureus bacteremia due to an intravascular device will continue to have fevers and positive blood cultures and be at an increased risk of dying unless the device is removed. As a general rule, when an appreciable quantity of pus, necrotic tissue, or a foreign body is present, the most effective treatment is an antimicrobial agent given in adequate dose plus a properly performed surgical procedure. Lack of Adequate Bacteriological Information One-half of the courses of antimicrobial therapy administered to hospitalized patients appear to be given in the absence of supporting microbiological data. Bacterial cultures and Gram stains of infected material are obtained too infrequently, and the results, when available, are often disregarded in the selection and application of drug therapy. Frequent use of drug combinations or drugs with the broadest spectra is a cover for diagnostic imprecision. The agents are selected more likely by habit than for specific indications, and the dosages employed are routine, rather than individualized on the basis of the clinical situation, microbiological information, and the pharmacological considerations presented in this and subsequent chapters of this section. For general information regarding infectious diseases, the reader is referred to the following chapters of Harrison's Principles of Internal Medicine, 16th ed., McGraw-Hill, New York, 2005: basic considerations in infectious disease (Chapters 104 to 108), issues regarding bacterial infections (Chapter 118), viral diseases (Chapters 161 and 162), fungal diseases (Chapter 182), and parasitic infections (Chapters 192 and 193). |
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 4416
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2025 . All rights reserved