| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Esophagogastrectomy and End-To-Side Esophagogastrostomy
This operation, together with adequate lymph node dissections, represents the procedure of choice for malignant lesions of the lower third of the esophagus. The dissection takes place through separate right (Ivor Lewis approachour preference) or left thoracic and abdominal midline incisions. In the chest, the esophagus is dissected to provide a satisfactory circumferential and longitudinal tumor-free margin, proximal to the lower third lesion. Mediastinal lymph node dissection is performed en bloc with the specimen. The transection of the esophagus, usually in its middle third, is controlled by intraoperative histological examination to ensure a tumor-free margin. In the abdomen, lymph node dissection of the celiac axis and its branches and splenectomy are performed as indicated, together with mobilization of a generous portion of gastric fundus, en bloc with the thoracic specimen.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
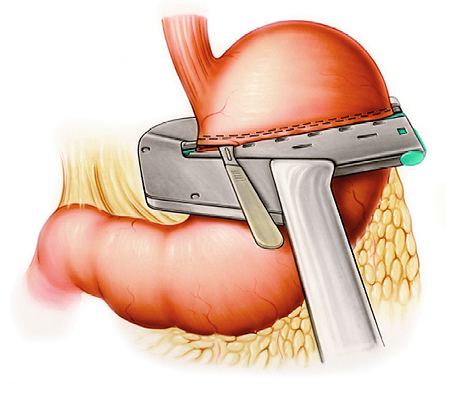
Step 1: Staple closure of the proximal and distal gastric fundus
Following mobilization of the distal esophagus and proximal stomach, the gastric fundus is stapled transversely at the level of planned resection with two applications of the TA 90 instrument. The first application is placed on the specimen side, followed by a second application distal and parallel to the previous staple line. Prior to removing the instrument used to place the second, caudad staple line, the stomach is transected along the superior edge of the TA 90 stapler.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
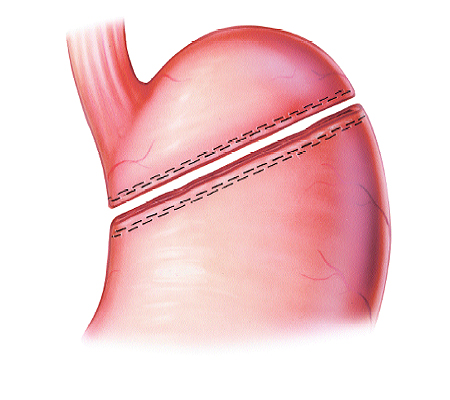
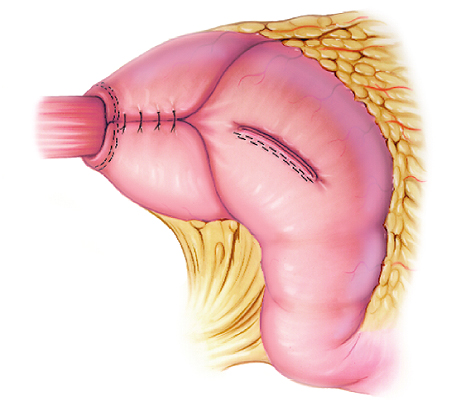
Step 2: Transection of the gastric fundus between the staple closures
Closure of both the remaining stomach and the specimen reduces the potential for intraperitoneal contamination.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
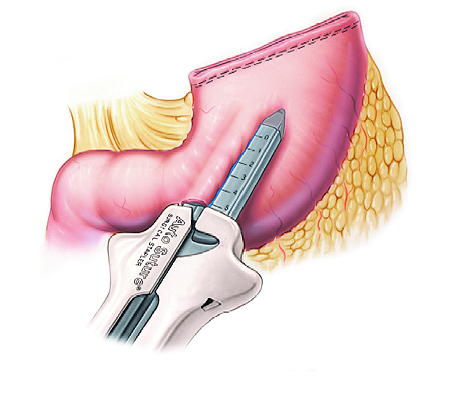
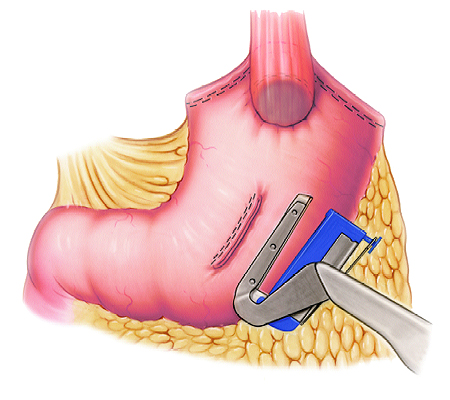
Step 3: Creation of a gastrotomy
A gastrotomy is performed with the GIA instrument. The anvil fork of the instrument is inserted into the gastric lumen through a 1 cm stab wound in the mid-to-lower third of the anterior wall of the remaining stomach at a minimum of 10 cm distal to the gastric closure. The cartridge-bearing fork is matched on the serosal surface to the intraluminal fork. The open instrument is advanced proximally over the distance that will accommodate the passage of the EEA instrument chosen for the esophagogastric anastomosis. The GIA halves are closed, the instrument is activated, and a gastrotomy with hemostatic edges is obtained.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
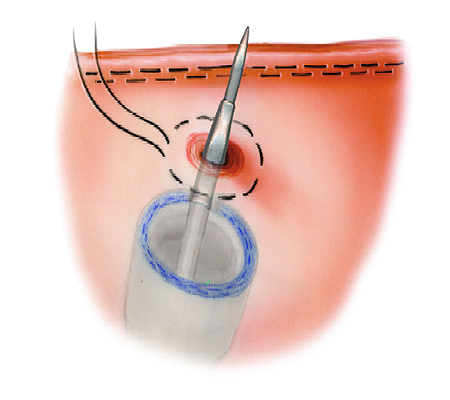
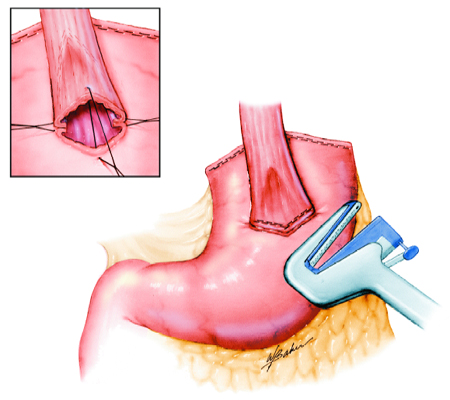
Step 4: Positioning of the EEA instrument, without anvil, in the gastric pouch at the site for the anastomosis.
The EEA instrument, without anvil, is inserted through the gastrotomy and positioned at the site chosen for anastomosis. The instrument is opened fully, allowing the tip of the center rod to perforate the anterior gastric wall 3 to 4 cm caudad to the stapled gastric closure. A manual purse-string suture is placed around the perforation site to prevent any serosal tearing or tissue slippage, and the suture is tied snugly, but not too tightly, around the center rod of the instrument.
Esophagogastrectomy and End-To-Side Esophagogastrostomy

Step 5: Placement of a purse-string suture on the esophagus and incision of the anterior wall
With gentle traction on the specimen, the PURSTRING instrument is positioned around the esophagus just proximal to the point of resection. A purse-string suture is placed. Prior to removal of the instrument, the anterior wall of the esophagus is incised along the inferior instrument edge.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
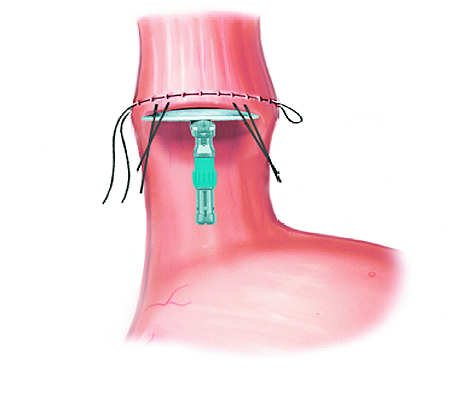
Step 6: Insertion of the EEA instrument anvil into the esophagus
After removing the PURSTRING instrument, stay sutures are placed at both ends of the transverse incision. While holding up the stay sutures of the anterior wall of the esophagus, to open its lumen, and exerting gentle downward traction on the specimen, the anvil of the EEA instrument is inserted into the esophagus.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
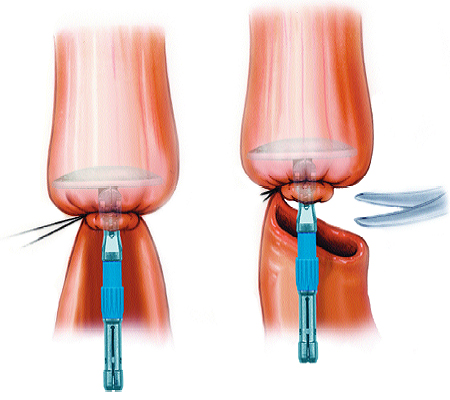
Step 7: Purse-string suture tied and resection of the esophagogastric specimen
The purse-string suture is tied firmly around the anvil shaft, and the posterior wall of the esophagus is transected, taking care not to compromise the integrity of the circular closure. The resection of the esophagogastric specimen is now complete.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
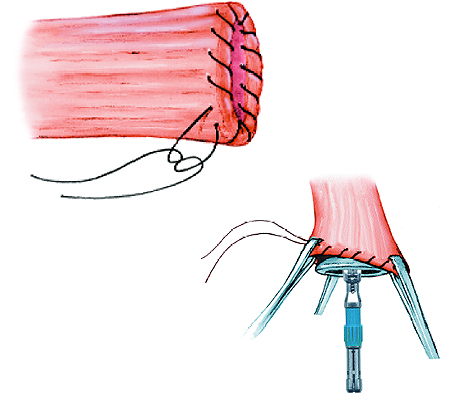
Step 8: Manual purse-string placement and insertion of the anvil following complete transection of the esophagus
If placement of the PURSTRING instrument is onerous because of limited exposure, the esophagus may be transected completely in a first step. The specimen is removed to free up space. The purse-string suture is then placed with a manual 2-0, monofilament, over-and-over full-thickness whipstitch, rounding the entire circumference of the esophageal stump, starting and ending at close points on the serosa. With the aid of three Allis clamps or stay sutures, placed equidistantly and holding open the rim of the esophagus, the anvil is advanced into the esophageal lumen and the purse-string suture is tied firmly around the anvil shaft.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
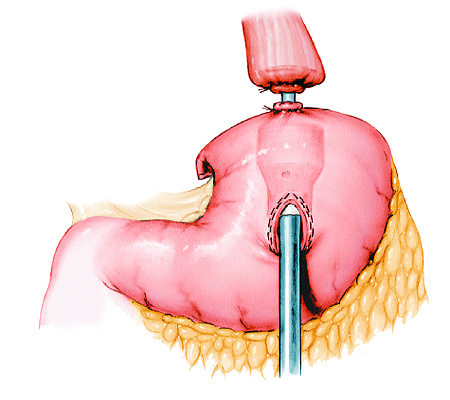
Step 9: Closure of the EEA instrument and end-to-side esophagogastrostomy
The anvil shaft and center rod of the EEA instrument are mated, and the instrument is closed, taking care that the tissue is snug against the cartridge and anvil and that no extraneous tissue is incarcerated between the stomach and esophagus.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
Step 10: Closure of the gastrotomy
Following completion of the end-to-side esophagogastrostomy, the circular stapling instrument is removed, the completeness of excised tissue donuts and the integrity of the anastomosis are verified, and the anterior gastrotomy is closed with a linear stapler.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
Step 11: Fundoplication
If the remaining stomach is wide and reaches the anastomosis with some redundancy in width and length, it is wrapped and sutured around the anastomosis in a modified Nissen mode to provide an antireflux mechanism to what is essentially a wide open conduit for acid or alkaline gastric juices to inundate and irritate the esophagus. An additional advantage of this gastric plication is the protection offered the anastomosis by coverage of the thick plicated gastric wall.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
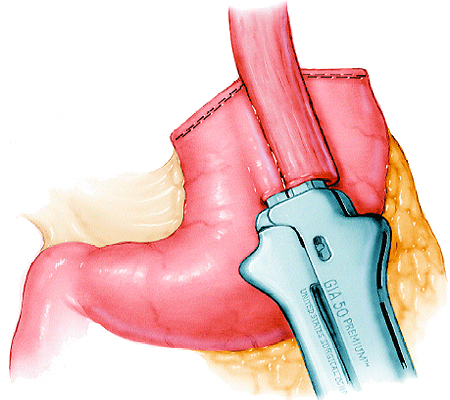
Step 12: Side-to-side esophagogastrostomy with the GIA instrument
Radical esophagogastrectomy should never be hostage to a single reconstructive technique of digestive tract continuity since the circumstances and difficulties encountered in each patient may require excisional strategies that would create a vacuum if only a single pattern of anatomical restoration was available. One alternative, of several proposed in this text, is esophagogastrostomy performed using the GIA instrument. For this anastomosis, the esophagus must be elevated from its bed over the length of the GIA instrument and placed on the anterior surface of the stomach. A 1 cm stab wound is made in the midanterior wall of the gastric remnant approximately 6 to 8 cm distal to the stapled gastric closure. The anvil fork of the GIA instrument is placed into the lumen of the stomach and the cartridge fork into the open-ended lumen of the esophagus. The tissue is evenly aligned on the forks of the instrument, which is then closed and activated.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
Step 13: Closure of the common opening
After removal of the instrument, the anastomosis is inspected for hemostasis. The linear staple lines joining the esophagus and stomach are held at the 3 oclock and 9 oclock positions of the now common GIA placement site by two everting stay sutures. A third suture is placed through the midpoints of the common opening, triangulating the circular rim of this opening as the midpoint suture is pulled tight.
Esophagogastrectomy and End-To-Side Esophagogastrostomy
Step 14: Completion of the anastomosis
As traction is placed on two consecutive stay sutures (e.g., 3 oclock and 6 oclock positions, 6 oclock and 9 oclock positions), the convex esophageal rim is placed against the concave gastric rim, forming semicircular pouting (everting) lips. These lips of esophageal wall above and gastric wall below are sutured in a cuneiform fashion with two applications of the TA 30 instrument, ensuring that all tissue layers and the ends of the previous placed staple lines are incorporated within these linear closures. The excess tissue is excised along the free edge of the linear stapler after each application, while preserving the midpoint stay suture between the first and the second application. This ensures complete closure of the entire semicircular pouting (everted) esophagogastric rims.
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 7047
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2025 . All rights reserved