| CATEGORII DOCUMENTE |
| Bulgara | Ceha slovaca | Croata | Engleza | Estona | Finlandeza | Franceza |
| Germana | Italiana | Letona | Lituaniana | Maghiara | Olandeza | Poloneza |
| Sarba | Slovena | Spaniola | Suedeza | Turca | Ucraineana |
Drugs Used for the Treatment of Myocardial Ischemia
Overview
|
This chapter briefly reviews the
pathophysiology underlying angina pectoris, the most common symptom of
chronic ischemic heart disease. The causes of the myocardial ischemia that
produces angina are defined in terms of the myocardial oxygen supplydemand
relationship. Stable and unstable angina, silent ischemia, variant angina,
and myocardial infarction are considered; the contributions of fixed
atherosclerotic coronary narrowings, of active coronary vasospasm, and of
intracoronary thrombosis in these syndromes are discussed to clarify the
roles of antianginal agents. Also discussed is the angina of autonomic
dysfunction, for which therapy must be specifically tailored to ameliorate
the underlying problem of great fluctuations in coronary perfusion pressure,
and in which conventional antianginal therapy is not efficacious. For each
class of antianginal therapy (organic nitrates, Ca2+ channel
antagonists, The use of organic nitrates (also covered in Chapter 34:
Pharmacological Treatment of Heart Failure) in sublingual, oral, buccal, and
intravenous forms is discussed, with attention to the issue of nitrate
tolerance and the relationship of nitrovasodilators to endogenous
endothelium-derived vasodilator(s). Interactions of organic nitrates with sildenafil
also are discussed. The multiple classes of Ca2+ channel
antagonists (also discussed in Chapter 33: Antihypertensive Agents and the
Drug Therapy of Hypertension) have distinct effects on vascular smooth muscle
and cardiac tissue, and these effects are placed in the context of the
ischemic cardiac syndromes. |
Drugs Used for the Treatment of Myocardial Ischemia: Introduction
|
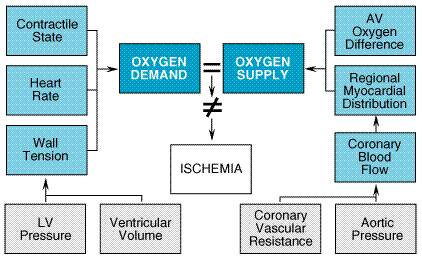
The primary symptom of ischemic heart disease is angina pectoris, caused by transient episodes of myocardial ischemia. These episodes of ischemia are due to an imbalance in the myocardial oxygen supplydemand relationship and may be caused by an increase in myocardial oxygen demand (determined by heart rate, ventricular wall tension, and ventricular contractility), by a decrease in myocardial oxygen supply (primarily determined by coronary blood flow, but occasionally modified by the oxygen-carrying capacity of the blood), or sometimes by both (Friesinger and Robertson, 1985, 1986; Kaplinsky, 1992; see Figure 321). Regardless of the precipitating factors, the sensation of angina is similar in most patients. Both typical and variant (Prinzmetal's) angina are commonly experienced as a heavy, pressing, substernal discomfort (rarely called 'pain'), often radiating to the left shoulder, flexor aspect of the left arm, jaw, or epigastrium, with a significant minority of patients noting discomfort in a different location or of a different character. Women, the elderly, and diabetics are more likely to have ischemia with atypical symptoms.
Angina pectoris is a common symptom, affecting 6,400,000 Americans (American Heart Association, 2001). It may occur in a stable pattern over many years or may become unstable, increasing in frequency or severity and even occurring at rest. In typical stable angina, the pathological substrate is usually fixed atherosclerotic narrowing of an epicardial coronary artery, upon which exertion, emotional stress, etc., superimpose an increase in myocardial oxygen consumption. In variant angina, focal or diffuse coronary vasospasm episodically reduces coronary flow. Patients also may display a mixed pattern of angina with the addition of altered vessel tone on a background of atherosclerotic narrowing. In the majority of patients with unstable angina, rupture of an atherosclerotic plaque, with consequent platelet adhesion and aggregation, decreases coronary blood flow. Plaques with thinner fibrous caps are recognized to be more 'vulnerable' to rupture (Fuster et al. 1996). Myocardial ischemia also may be 'silent,' with
electrocardiographic, echocardiographic, or radionuclide evidence of ischemia
appearing in the absence of symptoms. While some patients have only silent
ischemia, the majority of patients who have silent ischemia have symptomatic
episodes as well. The precipitants of silent ischemia appear to be the same
as those of symptomaticischemia. We now know that the 'ischemic
burden,'i.e., the total time a patient is ischemic each day, is
greater in many patients than was recognized previously. The agents that are
efficacious in conventional angina appear, in most trials, to be efficacious
in reducing silent ischemia. An unusual form of angina is seen in patients with autonomic dysfunction and faulty control of the circulation in the upright posture (Hines et al. 1981). The marked orthostatic hypotension seen in these patients can reduce coronary perfusion pressure sufficiently to cause myocardial ischemia even in patients with normal coronary arteries. As this form of angina is precipitated by upright posture and is relieved when the blood pressure and coronary perfusion pressure rise with sitting or lying, it may appear to be typical exertional angina if the history is not taken carefully and the blood pressure determined in the upright posture. The specific therapy needed for this form of angina is discussed below. This chapter describes the pharmacological agents used in the
treatment of angina. The major drugs are nitrovasodilators (see also Chapter
34: Pharmacological Treatment of Heart Failure), Antianginal agents may provide prophylactic or symptomatic treatment,
but |
Organic Nitrates
|
History Nitroglycerin was first synthesized in 1846 by Sobrero, who observed that a small quantity of the oily substance placed on the tongue elicited a severe headache. Constantin Hering, in 1847, developed the sublingual dosage form. In 1857, the eminent physician T. Lauder Brunton of Edinburgh administered amyl nitrite, a known vasodepressor, by inhalation and noted that anginal pain was relieved within 30 to 60 seconds. The action of amyl nitrite was transitory, however, and the dosage was difficult to adjust. Subsequently, William Murrell decided that the action of nitroglycerin mimicked that of amyl nitrite, and he established the use of sublingual nitroglycerin for relief of the acute anginal attack and as a prophylactic agent to be taken prior to exertion (Murrell, 1879). The empirical observation that organic nitrates could be used safely for the rapid, dramatic alleviation of the symptoms of angina pectoris led to their widespread acceptance by the medical profession. Basic investigations led to an understanding of the role of nitric oxide (Moncada et al., 1988) in both the vasodilation produced by nitrates and endogenous vasodilation. The importance of nitric oxide as a signaling molecule in the cardiovascular system and elsewhere was recognized by the awarding of the Nobel Prize in Medicine or Physiology to Furchgott, Ignarro, and Murad in 1998. Chemistry Organic nitrates are polyol esters of nitric acid, whereas organic nitrites are esters of nitrous acid (Table 321). Nitrate esters (CONO2) and nitrite esters (CONO) are characterized by a sequence of carbonoxygennitrogen, whereas nitro compounds possess carbonnitrogen bonds (CNO2). Thus, glyceryl trinitrate is not a nitro compound, and it is erroneously called nitroglycerin; however, this nomenclature is both widespread and official. Amyl nitrite is a highly volatile liquid that is administered by inhalation. Organic nitrates of low molecular mass (such as nitroglycerin) are moderately volatile, oily liquids, whereas the high-molecular-mass nitrate esters (e.g., erythrityl tetranitrate, pentaerythritol tetranitrate, isosorbide dinitrate) are solids. The fully nitrated polyols are lipid soluble, whereas their incompletely nitrated metabolites are more soluble in water. In the pure form (without an inert carrier such as lactose), nitroglycerin is explosive. The organic nitrates and nitrites and several other compounds that are capable of denitration to release nitric oxide (NO) have been collectively termed nitrovasodilators. Nitric oxide activates guanylyl cyclase, increasing intracellular levels of cyclic guanosine 3',5'-monophosphate (cyclic GMP), and thereby produces vasodilation (Murad, 1986; Molina et al., 1987; Thadani, 1992). Endogenous NO is formed when L-arginine is converted to citrulline by nitric oxide synthases. Both constitutive and inducible forms of these synthases are found in vascular endothelial and smooth muscle cells as well as in other cell types throughout the body, including the central nervous system (Lowenstein et al., 1994). In the setting of human atherosclerosis, the expression of endothelial nitric oxide synthase and the production of NO are reduced (Oemar et al., 1998). Pharmacological Properties Cardiovascular Effects Hemodynamic Effects The nitrovasodilators relax most smooth muscle, including that in arteries and veins. Low concentrations of nitroglycerin produce dilation of the veins that predominates over that of arterioles. Venodilation results in decreased left and right ventricular chamber size and end-diastolic pressures but little change in systemic vascular resistance. Systemic arterial pressure may fall slightly, and heart rate is unchanged or slightly increased reflexly. Pulmonary vascular resistance and cardiac output both are slightly reduced. Even doses of nitroglycerin that do not alter systemic arterial pressure often produce arteriolar dilation in the face and neck, resulting in a flush, or dilation of meningeal arterial vessels, causing headache. There is an enrichment of the enzyme that converts nitroglycerin to NO in venous compared to arterial smooth muscle cells, likely the basis of the partially venoselective properties of the nitrates (Bauer and Fung, 1996). Higher doses of organic nitrates cause further venous pooling and may decrease arteriolar resistance as well, decreasing systolic and diastolic blood pressure and cardiac output and resulting in pallor, weakness, dizziness, and activation of compensatory sympathetic reflexes. The resultant tachycardia and peripheral arteriolar vasoconstriction tend to restore systemic vascular resistance; this is superimposed on sustained venous pooling. Coronary blood flow may increase transiently as a result of coronary vasodilation, but with a subsequent decrease if cardiac output and blood pressure decrease sufficiently. In patients with autonomic dysfunction and an inability to increase sympathetic outflow (multiple-system atrophy and pure autonomic failure are the most common forms), the fall in blood pressure consequent to the venodilation produced by nitrates cannot be compensated. Nitrates may reduce arterial pressure and coronary perfusion pressure significantly and actually aggravate angina in addition to producing potentially life-threatening hypotension. The correct therapy in patients with orthostatic angina and normal coronary arteries is to correct the orthostatic hypotension by increasing volume retention (fludrocortisone and a high-sodium diet) by preventing venous pooling with fitted support garments and by the carefully titrated use of oral vasopressors. As patients with autonomic dysfunction occasionally may have coexistent coronary artery disease, the coronary anatomy should be defined before therapy is undertaken. Effects on Total and Regional Coronary Blood Flow Ischemia is a powerful stimulus to coronary vasodilation, and regional blood flow is adjusted by autoregulatory mechanisms. In the presence of atherosclerotic coronary narrowing, ischemia distal to the lesion is a stimulus for vasodilation, and, if the degree of narrowing is severe, much of the capacity to dilate is utilized to maintain resting blood flow. When situations arise that increase demand, further dilation may not be possible. After demonstration of direct coronary vasodilation in experimental animals, it became generally accepted that nitrates relieved anginal pain by dilating coronary arteries and thereby increasing coronary blood flow. This hypothesis was questioned by Gorlin and associates (1959), who were unable to demonstrate increases in coronary blood flow in patients with angina pectoris following the administration of nitroglycerin. However, organic nitrates do appear to cause redistribution of blood flow in the heart when the coronary circulation is partially occluded. Under these circumstances, there is a disproportionate reduction in blood flow to the subendocardial regions of the heart, which are subjected to the greatest extravascular compression during systole; organic nitrates tend to restore blood flow in these regions toward normal (Horwitz et al., 1971). The hemodynamic mechanisms responsible for these effects are not
entirely clear. Most hypotheses have focused on the ability of organic
nitrates to cause dilation and prevent vasoconstriction of large epicardial
vessels without impairing autoregulation in the small vessels, which are
responsible for about 90% of the overall coronary vascular resistance. The
vessel diameter is an important determinant of the response to nitroglycerin;
vessels larger than 200 In patients with angina due to coronary spasm, the ability of organic nitrates to dilate epicardial coronary arteries, and particularly regions affected by spasm, may be the primary mechanism by which they are of benefit. Effects on Myocardial Oxygen Requirements By their effects on the systemic circulation, the organic nitrates
also can reduce myocardial oxygen demand. The major determinants of
myocardial oxygen consumption include left ventricular wall tension, heart
rate, and the contractility of the myocardium. Ventricular wall tension is
affected by a number of factors that may be considered under the categories
of 'preload' and 'afterload.'Preload is determined
by the diastolic pressure that distends the ventricle (ventricular
end-diastolic pressure). Increasing end-diastolic volume augments the
ventricular wall tension (by the law of Organic nitrates do not directly alter the inotropic or chronotropic state of the heart. They do decrease both preload and afterload as a result of respective dilation of venous capacitance and arteriolar resistance vessels. Since the primary determinants of oxygen demand are reduced by the nitrates, their net effect usually is to decrease myocardial consumption of oxygen. In addition, an improvement in the lusitropic state of the heart may be seen, with more rapid early diastolic filling (Breisblatt et al., 1988). This may be secondary to the relief of ischemia, rather than primary, or may be due to a reflex increase in sympathetic activity. Nitrovasodilators also increase cyclic GMP in platelets with consequent inhibition of platelet function (De Caterina et al., 1988; Lacoste et al., 1994) and decreased deposition of platelets in animal models of arterial wall injury (Lam et al., 1988). While this may contribute to their antianginal efficacy, the effect appears to be modest and may in some settings be confounded by the potential of nitrates to alter the pharmacokinetics of heparin, reducing its antithrombotic effect. When nitroglycerin is injected or infused directly into the coronary circulation of patients with coronary artery disease, anginal attacks (induced by electrical pacing) are not aborted, even when coronary blood flow is increased. However, sublingual administration of nitroglycerin does relieve anginal pain in the same patients (Ganz and Marcus, 1972). Furthermore, venous phlebotomy that is sufficient to reduce left ventricular end-diastolic pressure can mimic the beneficial effect of nitroglycerin. Patients are able to exercise for considerably longer periods after the administration of nitroglycerin. Nevertheless, angina occurs, with or without nitroglycerin, at the same value of the 'triple product' (aortic pressure x heart rate x ejection time is proportional to the myocardial consumption of oxygen). The observation that angina occurs at the same level of myocardial oxygen consumption suggests that the beneficial effects of nitroglycerin are the result of a reduced cardiac oxygen demand, rather than an increase in the delivery of oxygen to ischemic regions of myocardium. However, these results do not preclude the possibility that a favorable redistribution of blood flow to ischemic subendocardial myocardium may contribute to relief of pain in a typical anginal attack, nor do they preclude the possibility that direct coronary vasodilation may be the major effect of nitroglycerin in situations where vasospasm compromises myocardial blood flow. Mechanism of Relief of Symptoms of Angina Pectoris Brunton ascribed the nitrate-induced relief of anginal pain to a decrease in cardiac work secondary to the fall in systemic arterial pressure. As described above, the ability of nitrates to dilate epicardial coronary arteries, even in areas of atherosclerotic stenosis, is modest, and the bulk of evidence continues to favor a reduction in myocardial work and thus in myocardial oxygen demand as their primary effect in chronic stable angina. Paradoxically, high doses of organic nitrates may reduce blood pressure to such an extent that coronary flow is compromised; reflex tachycardia and adrenergic enhancement of contractility also occur. These effects may override the salutary action of the drugs on myocardial oxygen demand and can aggravate ischemia. Additionally, sublingual nitroglycerin administration may produce bradycardia and hypotension, probably due to activation of the Bezold-Jarisch reflex (Gibbons et al., 1999). Other Effects The nitrovasodilators act on almost all smooth muscle. Bronchial smooth muscle is relaxed irrespective of the cause of the preexisting tone. The muscles of the biliary tract, including those of the gallbladder, biliary ducts, and sphincter of Oddi, are effectively relaxed. Smooth muscle of the gastrointestinal tract, including that of the esophagus, can be relaxed and its spontaneous motility decreased by nitrates both in vivo and in vitro. The effect may be transient and incomplete in vivo, but abnormal 'spasm' frequently is reduced. Indeed, many incidences of atypical chest pain and 'angina' are due to biliary or esophageal spasm, and these too can be relieved by nitrates. Similarly, nitrates can relax ureteral and uterine smooth muscle, but these effects are somewhat unpredictable. Mechanism of Action Nitrites, organic nitrates, nitroso compounds, and a variety of other nitrogen oxidecontaining substances (including nitroprusside; see Chapter 33: Antihypertensive Agents and the Drug Therapy of Hypertension) lead to the formation of the reactive free radical nitric oxide (NO), which can activate guanylyl cyclase and increase the synthesis of cyclic GMP in smooth muscle and other tissues (see Murad, 1986; Molina et al., 1987). The exact mechanism(s) of denitration of the organic nitrates, with the subsequent liberation of NO, is controversial (Harrison and Bates, 1993). A cyclic GMPdependent protein kinase catalyzes the phosphorylation of various proteins in smooth muscle. Eventually, the light chain of myosin is dephosphorylated (Waldman and Murad, 1987). Phosphorylation of the myosin light chain regulates the maintenance of the contractile state in smooth muscle. The pharmacological and biochemical effects of the nitrovasodilators appear to be identical to those of an endothelium-derived relaxing factor, which has been shown to be NO (Moncada et al., 1988; Ignarro et al., 1987; Murad, 1996; Furchgott, 1996). The relationship of endogenous nitric oxide to its precursor, L-arginine, has been reviewed (Moncada and Higgs, 1993). Nitric oxide appears to function as a biological signal in many cell types (Lowenstein et al., 1994; Vane, 1994). Absorption, Fate, and Excretion The biotransformation of organic nitrates is the result of reductive hydrolysis catalyzed by the hepatic enzyme glutathioneorganic nitrate reductase. The enzyme converts the lipid-soluble organic nitrate esters into more water-soluble denitrated metabolites and inorganic nitrite. The partially denitrated metabolites are considerably less potent vasodilators than are the parent compounds. However, under certain conditions their activity may become important. Since the liver has an enormous capacity to catalyze the reduction of organic nitrates, their biotransformation is a major factor in determining oral bioavailability and duration of action. The pharmacokinetic properties of nitroglycerin and isosorbide dinitrate have been studied in the greatest detail. Nitroglycerin One molecule of nitroglycerin reacts with two molecules of reduced glutathione to produce 1,3- or 1,2-glyceryl dinitrate and oxidized glutathione (Needleman, 1975). A comparison of the maximal velocities of metabolism of the clinically used nitrates by this reductase indicates that erythrityl tetranitrate is degraded three times faster than is nitroglycerin, while isosorbide dinitrate and pentaerythritol tetranitrate are denitrated at one-sixth and one-tenth the rate of nitroglycerin. In human beings, peak concentrations of nitroglycerin are found in plasma within 4 minutes of sublingual administration; the drug has a half-life of 1 to 3 minutes. The onset of action of nitroglycerin may be more rapid if it is delivered as a sublingual spray, rather than as a sublingual tablet (Ducharme et al., 1999). Dinitrate metabolites, which are about ten times less potent as vasodilators, appear to have a half-life of about 40 minutes. Isosorbide Dinitrate The major route of metabolism of isosorbide dinitrate in human beings is by enzymatic denitration followed by formation of glucuronide conjugates. Sublingual administration produces maximal concentrations of the drug in plasma by 6 minutes, and the fall in concentration is rapid (half-life approximately 45 minutes). The primary initial metabolites, isosorbide-2-mononitrate and isosorbide-5-mononitrate, have longer half-lives (3 to 6 hours) and are presumed to be responsible, at least in part, for the therapeutic efficacy of the drug. Isosorbide-5-Mononitrate This agent is available in tablet form. It has excellent bioavailability after oral administration as it does not undergo significant first-pass metabolism. It has a significantly longer half-life than does isosorbide dinitrate and has been formulated as a plain tablet and as a sustained-release preparation; both of which have longer durations of action than the corresponding dosage forms of isosorbide dinitrate. Correlation of Plasma Concentrations of Drug and Biological Activity Intravenous administration of nitroglycerin or the long-acting nitrates (isosorbide dinitrate, pentaerythritol tetranitrate, and erythrityl tetranitrate) in anesthetized animals produces the same transient (1 to 4 minutes) decrease in blood pressure. Relative to nitroglycerin, the potency of erythrityl tetranitrate as a vasodepressor in dogs is about 12% and that of isosorbide dinitrate 3.5%. Since denitration markedly reduces the activity of the organic nitrates, their rapid clearance from blood indicates that the transient duration of action under these conditions correlates with the concentrations of the parent compounds. The rate of hepatic denitration is characteristic of each nitrate and is influenced by hepatic blood flow or the presence of hepatic disease. In experimental animals, injection of moderate amounts of organic nitrates into the portal vein results in little or no vasodepressor activity, indicating that a substantial fraction of drug can be metabolized during its first circulation through the liver (isosorbide mononitrate is an exception). Tolerance Sublingual organic nitrates should be taken at the time of an anginal attack or in anticipation of exercise or stress. Such intermittent treatment results in reproducible cardiovascular effects. However, frequently repeated or continuous exposure to high doses of organic nitrates leads to a marked attenuation in the magnitude of most of their pharmacological effects (Anonymous, 1992; Thadani, 1992). The magnitude of tolerance is a function of dosage and the frequency of administration of the preparation. Tolerance may result from an inability of the vascular smooth muscle
to convert nitroglycerin to NO, 'true vascular tolerance,' or to
the activation of mechanisms extraneous to the vessel wall,
'pseudotolerance' (Munzel et al., 1996). Multiple mechanisms
have been proposed to account for nitrate tolerance, including volume
expansion, neurohumoral activation, cellular depletion of sulfhydryl groups,
and the generation of free radicals (Thadani, 1992; Rutherford, 1995; Parker
and Parker 1998). The administration of organic nitrates to healthy
volunteers is associated within 24 hours with the activation of the
renin-angiotensin-aldosterone system and with increases in plasma norepinephrine
(Parker et al., 1991). Clinical data relating to the ability of agents
that modify the renin-angiotensin-aldosterone system to prevent nitrate
tolerance are contradictory (Dakak et al., 1990; Muisan et al.,
1993; Parker and Parker 1993; Pizzulli et al., 1996; Heitzer et al.,
1998). Important factors that may influence the ability of angiotensin
converting enzyme (ACE) inhibitors to prevent nitrate tolerance and that can
influence the interpretation of clinical trials include the dose, treatment
with the ACE inhibitors prior to the initiation of nitrates, and the tissue
specificity of the agent. Despite the rationale for the depletion of
sulfhydryl groups leading to impaired biotransformation of nitrates to NO and
thereby resulting in nitrate tolerance, experimental results to date with
sulfhydryl donors have been disappointing. A more recent proposal has linked
nitroglycerin tolerance to endothelium-derived superoxide generation (Munzel et
al., 1995b). In the setting of patients with congestive heart failure,
administration of carvedilol, but not metoprolol, doxazosin, or
placebo, has resulted in the prevention of tolerance to the effects of
nitroglycerin on forearm blood flow (Watanabe et al., 1998). In
addition to its properties as an While these approaches appear to be effective, some patients develop an increased frequency of nocturnal angina when a nitrate-free interval is employed using nitroglycerin patches; such patients may need to receive another class of antianginal agent during this period. In addition, a phenomenon referred to as the 'zero-hour effect' has added to the complexity of designing an appropriate dosing regimen. In a 29-day study, the early morning exercise tolerance (before patch application) of patients using intermittent patch therapy was less than that of patients using placebo patches, though the antianginal efficacy of the patch itself was maintained (DeMots and Glasser, 1989). The clinical significance of this finding and its applicability to other dosage forms of nitroglycerin are not known. Tolerance does not appear to be a uniform phenomenon, as in some patients only partial tolerance seems to develop. The problem of anginal rebound during nitrate-free intervals is especially troublesome in the treatment of unstable angina with intravenous nitroglycerin. If coverage of the interval with other agents is ineffective, an alternative approach that often is used is to increase gradually the dose of intravenous nitroglycerin in an attempt to overcome tolerance. This approach has not been studied carefully. A special aspect of tolerance has been observed among individuals exposed to nitroglycerin in the manufacture of explosives. If protection is inadequate, workers may experience severe headaches, dizziness, and postural weakness during the first several days of employment. Tolerance then develops, but headache and other symptoms may reappear after a few days away from the jobthe 'Monday disease.' The most serious effect of chronic exposure is a form of organic nitrate dependence. Workers without demonstrable organic vascular disease have been reported to have an increase in the incidence of acute coronary syndromes during the 24- to 72-hour periods away from the work environment (Morton, 1977, Parker et al., 1995). Coronary and digital arteriospasm during withdrawal and its relaxation by nitroglycerin also have been demonstrated radiographically. Because of the potential problem of nitrate dependence, it seems prudent not to withdraw nitrates abruptly from a patient who has received such therapy chronically. Toxicity and Untoward Responses Untoward responses to the therapeutic use of organic nitrates are almost all secondary to actions on the cardiovascular system. Headache is common and can be severe. It usually decreases over a few days if treatment is continued and often can be controlled by decreasing the dose. Transient episodes of dizziness, weakness, and other manifestations associated with postural hypotension may develop, particularly if the patient is standing immobile, and may occasionally progress to loss of consciousness. This reaction appears to be accentuated by alcohol. It may be seen with very low doses of nitrates in patients with autonomic dysfunction. Even in the most severe nitrate syncope, positioning and other procedures to facilitate venous return are the only therapeutic measures required. It was widely believed that nitrates can increase intraocular pressure and precipitate glaucoma, but this fear appears to be unfounded (Robertson and Stevens, 1977). All of the organic nitrates occasionally can produce drug rash. Interaction of Nitrates with Sildenafil Erectile dysfunction is a frequently encountered problem, risk factors for which parallel those of coronary artery disease [diabetes mellitus, hypertension, known heart disease (Johannes et al., 2000) and a low level of high-density lipoprotein (Feldman et al., 1994)]. Thus, it is likely that many men requiring therapy for erectile dysfunction already may be receiving (or may require, especially if they increase physical activity) antianginal therapy. The past decade has seen remarkable advances in our understanding of the physiology of penile erection (Andersson and Wagner, 1995). Cells in the corpus cavernosum produce nitric oxide during sexual arousal in response to nonadrenergic, noncholinergic neurotransmission (Kim et al., 1991; Rajfer et al., 1992; and Burnett et al., 1992). Nitric oxide stimulates the formation of cyclic GMP, which leads to relaxation of smooth muscle of the corpus cavernosum and penile arteries. The accumulation of cyclic GMP can be enhanced by inhibition of the cyclic GMP-specific phopshophodiesterase-5 (PDE5) family (Beavo et al., 1994). Sildenafil (VIAGRA) was developed as an inhibitor of PDE5 (Boolell et al., 1996) and has been demonstrated to improve erectile function in patients with various causes of erectile dysfunction (Goldstein et al., 1998). The side effects of sildenafil are largely predictable on the basis of
its effects on PDE5. Headache, flushing, and rhinitis may be observed, as may
dyspepsia due to relaxation of the lower esophageal sphincter, all thought to
be consequences of the inhibition of PDE5. Sildenafil also is a weak
inhibitor of PDE6, the isoenzyme involved in photoreceptor signal
transduction (Beavo et al., 1994), and sildenafil has been associated
with visual disturbances, most notably changes in the perception of color hue
or brightness (Wallis et al., 1999; Goldstein et al., 1998).
Sildenafil's most important toxicity is hemodynamic. When given alone to men
with severe coronary artery disease, sildenafil has modest effects on blood
pressure, producing less than a 10% fall in systolic, diastolic, and mean
systemic pressures and in pulmonary artery systolic and mean pressures (Herrmann
et al., 2000). However, it has a significant and potentially dangerous
interaction with nitrates. As discussed above, the therapeutic actions of
organic nitrates are mediated via their conversion to NO with
resultant increases in cyclic GMP. In the presence of a PDE5 inhibitor, nitrates
cause profound increases in cyclic GMP and can produce dramatic reductions in
blood pressure. Healthy male subjects pretreated with sildenafil exhibited a
much greater decrease in systolic blood pressure when treated with sublingual
glyceryl trinitrate, and in many a fall of more than 25 mm Hg was detected (Webb
et al., 1999). This interaction between sildenafil and nitrates is the
basis for the warning that sildenafil should not be prescribed to patients
receiving any form of nitrate (Cheitlen et al., 1999) and dictates
that patients should be questioned about the use of sildenafil within 24
hours before nitrates are administered. A period of longer than 24 hours may
be needed after sildenafil for safe use of nitrates. In the event that
patients develop significant hypotension following combined administration of
sildenafil and a nitrate, fluids and Sildenafil is metabolized via CYP3A4, and its toxicity may be
enhanced in patients who receive other substrates of this enzyme, including
macrolide and imidazole antibiotics, some HMG-CoA reductase inhibitors, and
highly active antiretroviral therapy (HAART; see Chapter 51:
Antiretroviral Agents: Antiretroviral Agents) (Hall and Ahmad, 1999).
Sildenafil also has been demonstrated to prolong cardiac repolarization by
blocking the IKr (Geelen et al., 2000). Although these
interactions and effects are clinically important, the overall incidence and
profile of adverse events observed with sildenafil, when used without
nitrates, are consistent with the expected background frequency of the same
events in the treated population (Zusman et al., 1999). In patients
with coronary artery disease who are not currently taking nitrates and whose
exercise capacity indicates that usual sexual activity is unlikely to
precipitate angina, the use of sildenafil can be considered. Such therapy
needs to be individualized and appropriate warnings given about the risk of
toxicity if nitrates are taken during the next 24 hours for angina.
Alternative nonnitrate antianginal therapy, such as Therapeutic Uses Angina Diseases that predispose to angina should be treated as part of a comprehensive therapeutic program with the primary goal being to prolong life. Such conditions as hypertension, anemia, thyrotoxicosis, obesity, heart failure, cardiac arrhythmias, and acute anxiety can precipitate anginal symptoms in many patients. The patient should be asked to stop smoking and overeating, hypertension and hyperlipidemia should be corrected (see Chapters 33: Antihypertensive Agents and the Drug Therapy of Hypertension and 36: Drug Therapy for Hypercholesterolemia and Dyslipidemia), and daily aspirin (or a thienopyridine such as clopidogrel or ticlopidine, if aspirin is not tolerated; see Chapter 55: Anticoagulant, Thrombolytic, and Antiplatelet Drugs) should be prescribed. Exposure to sympathomimetic agents (e.g., those in nasal decongestants) should be avoided. The use of drugs that modify the perception of pain is a poor approach to the treatment of angina, since the underlying myocardial ischemia is not relieved. See Table 321 for preparations and dosages of the nitrites and organic nitrates. The rapidity of onset, the duration of action, and the likelihood of developing tolerance are related to the method of administration. Sublingual Administration Because of its rapid action, long-established efficacy, and low cost, nitroglycerin is the most useful drug among the organic nitrates that can be given sublingually. The onset of action is within 1 to 2 minutes, but the effects are undetectable by 1 hour after administration. An initial dose of 0.3 mg of nitroglycerin often will relieve pain within 3 minutes. Absorption may be limited in patients with dentures or with dry mouths. Tablets of nitroglycerin are stable but should be dispensed in glass containers and protected from moisture, light, and extremes of temperature. Active tablets usually produce a burning sensation under the tongue, but the absence of a burning sensation does not reliably predict loss of activity. Patients, especially elderly ones, differ in the ability to detect the burning sensation. Anginal pain may be prevented when the drug is used prophylactically immediately prior to exercise or stress. The smallest effective dose should be prescribed. Patients should be taught to seek medical attention immediately when three tablets taken over a 15-minute period do not relieve a sustained attack, since this situation may be indicative of myocardial infarction or another cause of the pain. The patient also should be advised that there is no virtue in trying to avoid taking sublingual nitroglycerin for anginal pain. Other nitrates that can be taken sublingually do not appear to be longer acting than nitroglycerin, as their half-lives depend only on the rate at which they are delivered to the liver. They are not more effective than nitroglycerin and often are more expensive. Oral Administration Oral nitrates often are used to provide prophylaxis against anginal episodes in patients who have more than occasional angina. They must be given in sufficient dosage to provide effective plasma levels after first-pass hepatic degradation. At low doses (e.g., 5 to 10 mg of isosorbide dinitrate) they are no more effective than placebo in decreasing the frequency of angina or increasing the patient's exercise tolerance. Clinical studies that have used higher doses of either isosorbide dinitrate (e.g., 20 mg or more orally every 4 hours) or sustained-release preparations of nitroglycerin indicate that such regimens decrease the frequency of attacks of angina and improve exercise tolerance. Effects peak at 60 to 90 minutes and last for 3 to 6 hours. Under these circumstances, the activities of less potent metabolites also may contribute to the therapeutic effect. Chronic oral administration of isosorbide dinitrate (120 to 720 mg daily) results in persistence of the parent compound and higher concentrations of metabolites in plasma. However, these doses are more likely to cause troublesome side effects and tolerance. Significant, prolonged (up to 4 hours) improvement of exercise tolerance also can be demonstrated with a sustained-release oral form of nitroglycerin, but high doses (e.g., 6.5 mg) of nitroglycerin are required. Cutaneous Administration Application of nitroglycerin ointment can relieve angina, prolong exercise capacity, and reduce ischemic ST depression with exercise for 4 hours or more. Nitroglycerin ointment (2%) is applied to the skin [2.5 to 5 cm (1 to 2 in.) as it is squeezed from the tube; it is then spread in a uniform layer]; the dosage must be adjusted for each patient. Effects are apparent within 30 to 60 minutes (although absorption is variable) and last for 4 to 6 hours. The ointment is particularly useful for controlling nocturnal angina, which commonly develops within 3 hours after the patient goes to sleep. Transdermal nitroglycerin discs utilize a nitroglycerin-impregnated polymer (bonded to an adhesive bandage) that permits gradual absorption and a continuous plasma nitrate concentration over 24 hours. The onset of action is slow, with peak effects occurring at 1 to 2 hours. To avoid tolerance and loss of the therapeutic effect, therapy should be interrupted for at least 8 hours each day. With this regimen, long-term prophylaxis of ischemic episodes often can be attained. Transmucosal or Buccal Nitroglycerin This formulation is inserted under the upper lip above the incisors, where it adheres to the gingiva and gradually dissolves in a uniform manner. Hemodynamic effects are seen within 2 to 5 minutes, and it is therefore useful for short-term prophylaxis of angina. Nitroglycerin continues to be released into the circulation for a prolonged period, and exercise tolerance may be enhanced for up to 5 hours. Congestive Heart Failure The utility of nitrovasodilators to relieve pulmonary congestion and to increase cardiac output in congestive heart failure is well established and is addressed in Chapter 34: Pharmacological Treatment of Heart Failure. Unstable Angina Unstable angina has been considered a single entity in most therapeutic trials; it has included patients with new-onset exertional angina, with an increase in their usual pattern of angina, and with rest angina, with or without a preceding history of exertional angina. The electrocardiogram (ECG) may show either elevation or depression of the ST segment, with variable T-wave abnormalities. In patients with left main or three-vessel disease, revascularization leads to improved survival (Multicenter Study, 1978). In the remainder of patients, and in all patients prior to determination of the coronary anatomy, appropriate medical therapy provides important benefits. The pathophysiology in most patients studied involves thrombosis overlying a ruptured atherosclerotic plaque. However, there is some variability in the anatomic substrate of unstable angina, with gradually progressive atherosclerosis accounting for some cases of new-onset exertional angina, and vasospasm occurring in minimally atherosclerotic coronary vessels accounting for some cases where rest angina has never been preceded by or associated with exertional angina. It is likely that this variability accounts for the differences in therapeutic response seen in studies with differing inclusion criteria. Multiple agents are employed in the acute phase of treatment, although few have been demonstrated conclusively to reduce mortality. Aspirin (see below), by inhibiting platelet aggregation, has been shown clearly to improve survival (Kerins and FitzGerald, 1991). Heparin (either unfractionated or low-molecular-weight heparin) also appears to reduce angina and prevent infarction. These and related agents are discussed in detail in Chapters 27: Analgesic-Antipyretic and Antiinflammatory Agents and Drugs Employed in the Treatment of Gout and 55: Anticoagulant, Thrombolytic, and Antiplatelet Drugs. Nitrates are useful in reducing vasospasm and controlling angina; their administration should be initiated intravenously. Intravenous administration of nitroglycerin allows high concentrations of drug to be attained rapidly. As nitroglycerin is promptly degraded, the plasma concentration can be titrated quickly and safely using this route. If coronary vasospasm is present, intravenous nitroglycerin is likely to be effective, although the addition of a Ca2+ channel blocker is required to achieve complete control in some patients. Because of the potential risks of profound hypotension, nitrates should be withheld and alternate antianginal therapy administered if patients have consumed sildenafil within the prior 24 hours (see above). Myocardial Infarction Therapeutic maneuvers in myocardial infarction are directed at reducing the ultimate size of the infarct and preserving or retrieving viable tissue by reducing the oxygen demand of the myocardium. Since the proximate cause of myocardial infarction is intracoronary thrombosis, reperfusion therapies are critically important and include thrombolytic agents and direct percutaneous coronary angioplasty (Ryan et al., 1999). Thrombolytic and antiplatelet therapy are discussed in Chapter 55: Anticoagulant, Thrombolytic, and Antiplatelet Drugs. A drug that favorably alters the oxygen balance could decrease the area of myocardial damage if it were given soon after infarction. In the past, nitroglycerin was considered to be contraindicated for use in patients with acute myocardial infarction because of its ability to induce hypotension and reflex tachycardia, although it may be highly efficacious if the infarction is due to prolonged coronary spasm. Nevertheless, evidence that nitrates improve mortality in myocardial infarction is sparse. Nitrates may be most helpful in patients in whom reperfusion does not occur, despite thrombolytic agents, and may prevent adverse remodeling. The effects of nitrates in patients with acute myocardial infarction were assessed in two large trials (GISSI-3, 1994, and ISIS-4 Collaborative Group, 1995). In the GISSI-3 study, 19,394 patients with acute myocardial infarction were randomized to receive either transdermal nitroglycerin (10 mg daily with a 10-hour nitrate-free interval overnight) or placebo for 6 weeks. There were no significant effects of nitroglycerin on mortality, reinfarction, revascularization procedures, or renal dysfunction. There was a slight reduction in postinfarction angina in the nitroglycerin-treated group (20.7% vs. 19.7%). A similar lack of benefit on mortality was observed in the ISIS-4 study of 58,050 patients, some of whom were randomized to receive an oral controlled-release form of isosorbide mononitrate, 60 mg each morning for 28 days, or placebo. In the ISIS-4 study there was no effect of the nitrate on postinfarction angina. Thus transdermal or oral nitrates are safe and well tolerated in the setting of myocardial infarction and may have a beneficial effect on pain, but they do not provide a survival advantage. Variant (Prinzmetal's) Angina The large coronary arteries normally contribute little to coronary
resistance. However, in variant angina, coronary constriction results in
reduced blood flow and ischemic pain. Multiple mechanisms have been
hypothesized to be involved in the initiation of vasospasm, including
endothelial cell injury (Freisinger and Robertson, 1986). It does not seem
likely that abnormalities of sympathetic input are etiologic (Robertson et
al., 1979), and |
Ca2+ Channel Antagonists
|
History The work in the 1960s of Fleckenstein, Godfraind, and their colleagues led to the concept that drugs can alter cardiac and smooth muscle contraction by blocking the entry of Ca2+ into myocytes. Godfraind and associates showed that the ability of the diphenylpiperazine analogs cinnarizine and lidoflazine to prevent vascular smooth muscle contraction induced by some agonists could be overcome by raising the concentration of Ca2+ in the extracellular medium; they used the term 'calcium antagonist' to describe these agents (see Godfraind and Kaba, 1972; Godfraind et al., 1986). Hass and Hartfelder reported in 1962 that verapamil, a putative coronary vasodilator, possessed negative inotropic and chronotropic effects that were not seen with other vasodilatory agents, such as nitroglycerin. In 1967, Fleckenstein suggested that the negative inotropic effect resulted from inhibition of excitationcontraction coupling and that the mechanism involved reduction of the movement of Ca2+ into cardiac myocytes (see Fleckenstein, 1983). A derivative of verapamil, gallopamil, and other compounds, such as nifedipine (Kohlhardt and Fleckenstein, 1977), also were shown to block the movement of Ca2+ through the cardiac myocyte Ca2+ channel, or the slow channel (see Chapter 35: Antiarrhythmic Drugs), and thereby alter the plateau phase of the cardiac action potential. Subsequently, many drugs in several chemical classes have been shown to alter cardiac and smooth muscle contraction by blocking or 'antagonizing' the entry of Ca2+ through channels in the myocyte membrane. Chemistry The ten Ca2+ channel antagonists that have been approved
for clinical use in the Pharmacological Properties Cardiovascular Effects Actions in Vascular Tissue Although there is some involvement of Na+ currents, depolarization of vascular smooth muscle cells is primarily dependent on the influx of Ca2+ (Bolton, 1979). At least three distinct mechanisms may be responsible for contraction of vascular smooth muscle cells. First, voltage-sensitive Ca2+ channels open in response to depolarization of the membrane, and extracellular Ca2+ moves down its electrochemical gradient into the cell. After closure of Ca2+ channels, a finite period of time is required before the channels can open again in response to a stimulus. Second, agonist-induced contractions that occur without depolarization of the membrane result from the hydrolysis of membrane phosphatidylinositol with the formation of inositol trisphosphate, which acts as a second messenger to release intracellular Ca2+ from the sarcoplasmic reticulum (see Berridge, 1993). This receptor-mediated release of intracellular Ca2+ may trigger further influx of extracellular Ca2+. Third, receptor-operated Ca2+ channels allow the entry of extracellular Ca2+ in response to receptor occupancy. An increase in cytosolic Ca2+ results in enhanced binding of Ca2+ to the protein calmodulin. The Ca2+calmodulin complex in turn activates myosin light-chain kinase, with resultant phosphorylation of the light chain of myosin. Such phosphorylation promotes interaction between actin and myosin and contraction of smooth muscle. Ca2+ channel antagonists or blockers inhibit the voltage-dependent Ca2+ channels in vascular smooth muscle at significantly lower concentrations than are required to interfere with the release of intracellular Ca2+ or to block receptor-operated Ca2+ channels. All Ca2+ channel blockers relax arterial smooth muscle, but they have little effect on most venous beds and hence do not affect cardiac preload significantly. Actions in Cardiac Cells The mechanisms involved in excitationcontraction coupling in the heart differ from those in vascular smooth muscle in that a portion of the two inward currents is carried by Na+ through the fast channel in addition to that carried by Ca2+ through the slow channel. In the sinoatrial (SA) and atrioventricular (AV) nodes, depolarization is largely dependent on the movement of Ca2+ through the slow channel. Within the cardiac myocyte, Ca2+ binds to troponin, the inhibitory effect of troponin on the contractile apparatus is relieved, and actin and myosin interact to cause contraction. Thus, Ca2+ channel blockers can produce a negative inotropic effect. Although this is true of all classes of Ca2+ channel blockers, the greater degree of peripheral vasodilation seen with the dihydropyridines is accompanied by sufficient baroreflex-mediated increase in sympathetic tone to overcome the negative inotropic effect. Diltiazem also may inhibit mitochondrial Na+Ca2+ exchange (Schwartz, 1992). The effect of a Ca2+ channel blocker on atrioventricular conduction and on the rate of the sinus node pacemaker is dependent on whether or not the agent delays the recovery of the slow channel (Henry, 1983). Although nifedipine reduces the slow inward current in a dose-dependent manner, it does not affect the rate of recovery of the slow Ca2+ channel (Kohlhardt and Fleckenstein, 1977). The channel blockade caused by nifedipine and related dihydropyridines also shows little dependence on the frequency of stimulation. At doses used clinically, nifedipine does not affect conduction through the node. In contrast, verapamil not only reduces the magnitude of the Ca2+ current through the slow channel but also decreases the rate of recovery of the channel. In addition, channel blockade caused by verapamil (and to a lesser extent by diltiazem) is enhanced as the frequency of stimulation increases, a phenomenon known as 'frequency dependence' or 'use dependence.' Verapamil and diltiazem depress the rate of the sinus node pacemaker and slow AV conduction; the latter effect is the basis for their use in the treatment of supraventricular tachyarrhythmias (see Chapter 35: Antiarrhythmic Drugs). Bepridil, like verapamil, inhibits both slow inward Ca2+ current and fast inward Na+ current. It has a direct negative inotropic effect. Its electrophysiologic properties lead to slowing of the heart rate, prolongation of the AV nodal effective refractory period, and, importantly, prolongation of the QTc interval. Particularly in the setting of hypokalemia, the last effect can be associated with torsades de pointes, a potentially lethal ventricular arrhythmia (see Chapter 35: Antiarrhythmic Drugs). Hemodynamic Effects All of the Ca2+ channel blockers that have been approved for clinical use decrease coronary vascular resistance and increase coronary blood flow. The dihydropyridines are more potent vasodilators in vivo and in vitro than is verapamil, which is more potent than diltiazem. The hemodynamic effects of each of these agents vary, depending on the route of administration and the extent of left ventricular dysfunction. Nifedipine given intravenously increases forearm blood flow with little effect on venous pooling; this indicates a selective dilation of arterial resistance vessels. The decrease in arterial blood pressure elicits sympathetic reflexes, with resultant tachycardia and positive inotropy. Nifedipine also has direct negative inotropic effects in vitro. However, nifedipine relaxes vascular smooth muscle at significantly lower concentrations than those required for prominent direct effects on the heart. Thus, arteriolar resistance and blood pressure are lowered, contractility and segmental ventricular function are improved, and heart rate and cardiac output are increased modestly (Serruys et al., 1981; Theroux et al., 1980). After oral administration of nifedipine, arterial dilation increases peripheral blood flow; venous tone does not change. The other dihydropyridinesnicardipine, amlodipine, isradipine, felodipine,
nisoldipine, and nimodipineshare many of the cardiovascular effects of nifedipine.
There may be some selectivity of nicardipine for coronary vessels compared
with peripheral vessels (Pepine and Lambert, 1988); in comparative studies,
nicardipine appears to produce fewer side effects, such as dizziness, than
does nifedipine but has equivalent antianginal efficacy (DeWood and Wohlbach,
1990). Intravenous or oral administration of nicardipine results in decreases
in systolic and diastolic blood pressure that are accompanied by an increase
in cardiac output because of the reduction in afterload and compensatory
increases in heart rate and ejection fraction. It also appears to reduce left
ventricular diastolic dysfunction (Hanet et al., 1990). Nicardipine
decreases the frequency of anginal attacks and improves exercise tolerance in
patients with effort-induced angina (Pepine and Lambert, 1988). Amlodipine is
a dihydropyridine that has slow absorption and a prolonged effect. With a
plasma half-life of 35 to 50 hours, plasma levels and effect increase over 7
to 10 days of therapy. Amlodipine produces both peripheral arterial
vasodilation and coronary dilation, with a hemodynamic profile similar to
that of nifedipine. However, there is less reflex tachycardia with
amlodipine, possibly because the long half-life produces minimal peaks and
troughs in plasma concentrations (van Zwieten and Pfaffendorf, 1993; Bepridil has been demonstrated to reduce blood pressure and heart rate in patients with stable exertional angina. It also produces an increase in left ventricular performance in patients with angina, but its side-effect profile (see below) limits its use to truly refractory patients (Zusman et al., 1993; Hollingshead et al., 1992). Verapamil is a less potent vasodilator in vivo than are the dihydropyridines. Like the latter agents, verapamil causes little effect on venous resistance vessels at concentrations that produce arteriolar dilation. With doses of verapamil sufficient to produce peripheral arterial vasodilation, there are more direct negative chronotropic, dromotropic, and inotropic effects than with the dihydropyridines. Intravenous verapamil causes a decrease in arterial blood pressure due to a decrease in vascular resistance, but the reflex tachycardia is blunted or abolished by the direct negative chronotropic effect of the drug. The intrinsic negative inotropic effect of verapamil is partially offset by both a decrease in afterload and the reflex increase in adrenergic tone. Thus, in patients without congestive heart failure, ventricular performance is not impaired and may actually improve, especially if ischemia is limiting performance. In contrast, in patients with congestive heart failure, intravenous verapamil can cause a marked decrease in contractility and left ventricular function. Oral administration of verapamil results in reduction of peripheral vascular resistance and blood pressure with no change in heart rate (Theroux et al., 1980). The relief of pacing-induced angina seen with verapamil is due primarily to a reduction in myocardial oxygen demand (Rouleau et al., 1983). Intravenous administration of diltiazem can result initially in a marked decrease in peripheral vascular resistance and arterial blood pressure, which elicits a reflex increase in heart rate and cardiac output. Heart rate then falls below initial levels because of the direct negative chronotropic effect of the agent. Oral administration of diltiazem results in a sustained fall in both heart rate and mean arterial blood pressure (Theroux et al., 1980). Despite the fact that diltiazem and verapamil produce similar effects on the SA and AV nodes, the negative inotropic effect of diltiazem is more modest. The effect of Ca2+ channel blockers on diastolic ventricular relaxation (the lusitropic state of the ventricle) is complex. The direct effect of several of these agents, assessed when they are given by the intracoronary route, is to impair relaxation (Rousseau et al., 1980; Amende et al., 1983; Serruys et al., 1983; Walsh and O'Rourke, 1985). Although several clinical studies have suggested an improvement in peak left ventricular filling rates when verapamil, nifedipine, nisoldipine, or nicardipine was given systemically (Bonow et al., 1982; Paulus et al., 1983; Rodrigues et al., 1987; DEFIANT-II Research Group, 1997), one must be cautious in extrapolating this change in filling rates to enhancement of relaxation. Indeed, in studies by Nishimura et al. (1993), verapamil increased peak filling rate but also increased left ventricular end-diastolic pressure. Because ventricular relaxation is modulated at several levels (Brutsaert et al., 1993), the effect of even a single agent may be complex. If reflex stimulation of sympathetic tone increases myocardial cyclic AMP levels, increased lusitropy will result and may outweigh a direct negative lusitropic effect. Likewise, a reduction in afterload will improve the lusitropic state. In addition, if ischemia is improved, the negative lusitropic effect of asymmetrical left ventricular contraction will be reduced. However, in any given patient, the sum total of these effects cannot be determined a priori. Thus, caution should be exercised in the use of Ca2+ channel blockers for this purpose; it is ideal if the end result can be determined objectively before committing the patient to therapy. Mechanisms of Action Increased concentrations of cytosolic Ca2+ cause increased contraction of cardiac and vascular smooth muscle cells. The entry of extracellular Ca2+ is more important in initiating the contraction of myocardial cells, while the release of Ca2+ from intracellular storage sites also participates in contraction of vascular smooth muscle, particularly in some vascular beds. In addition, the entry of extracellular Ca2+ can trigger the release of additional Ca2+ from intracellular stores. Cytosolic Ca2+ concentrations may be increased by various contractile stimuli. Thus, many hormones and neurohormones increase Ca2+ influx through so-called receptor-operated channels, while high external concentrations of K+ and depolarizing electrical stimuli increase Ca2+ influx through voltage-sensitive, or 'potential-operated,' channels (Bevan et al., 1982). Voltage-sensitive channels contain domains of homologous sequence that
are arranged in tandem within a single large subunit. In addition to the
major channel-forming subunit (termed Voltage-sensitive Ca2+ channels have been divided into at
least three subtypes based on their conductances and sensitivities to voltage
(Schwartz, 1992; Tsien et al., 1988). The channels best characterized
to date are the L, N, and T subtypes, although P/Q and R channels have been
identified. Only the L-type channel is sensitive to the dihydropyridine Ca2+
channel blockers. Large divalent cations such as Cd2+ and Mn2+
block a wider range of Ca2+ channels. All approved Ca2+
channel blockers bind to the The vascular and cardiac effects of some of the Ca2+ channel blockers are summarized below and in Table 322. Absorption, Fate, and Excretion Although the absorption of these agents is nearly complete after oral administration, their bioavailability is reduced, in some cases markedly, because of first-pass hepatic metabolism. The effects of these drugs are evident within 30 to 60 minutes of an oral dose, with the exception of the more slowly absorbed and longer-acting agents amlodipine, isradipine, and felodipine. For comparison, peak effects of verapamil occur within 15 minutes of its intravenous administration. These agents all are bound to plasma proteins to a significant extent (70% to 98%); their elimination half-lives are widely variable and may range from 1.3 to 64 hours. During repeated oral administration, bioavailability and half-life may increase because of saturation of hepatic metabolism. A major metabolite of diltiazem is desacetyldiltiazem, which has about one-half of diltiazem's potency as a vasodilator. N-Demethylation of verapamil results in production of norverapamil, which is biologically active but much less potent than the parent compound. The half-life of norverapamil is about 10 hours. The metabolites of the dihydropyridines are inactive or weakly active. In patients with hepatic cirrhosis, the bio availabilities and half-lives of the Ca2+ channel blockers may be increased, and dosage should be decreased accordingly. The half-lives of these agents also may be longer in older patients. Except for diltiazem and nifedipine, all of the Ca2+ channel blockers are administered as racemic mixtures (Abernethy and Schwartz, 1999). Toxicity and Untoward Responses The most common side effects caused by the Ca2+ channel antagonists, particularly the dihydropyridines, are due to excessive vasodilation. These effects may be expressed as dizziness, hypotension, headache, flushing, digital dysesthesia, and nausea. Patients also may experience constipation, peripheral edema, coughing, wheezing, and pulmonary edema. Nimodipine may produce muscular cramps when given in the large doses required for a beneficial effect in patients with subarachnoid hemorrhage. Less common side effects include rashes, somnolence, and occasional minor elevations of liver function tests. These side effects usually are benign and may abate with time or with adjustment of the dose. Aggravation of myocardial ischemia has been observed in two studies with the dihydropyridine nifedipine (Schulz et al., 1985; Egstrup and Anderson, 1993). In both of these studies, worsening of angina was observed in patients with an angiographically demonstrable coronary collateral circulation. The worsening of angina may have resulted from excessive hypotension and decreased coronary perfusion, selective coronary vasodilation in nonischemic regions of the myocardium (i.e., coronary steal, since vessels perfusing ischemic regions may already be maximally dilated), or an increase in oxygen demand owing to increased sympathetic tone and excessive tachycardia. In a study of monotherapy with an immediate-release formulation of nisoldipine, the dihydropyridine was not superior to placebo therapy and was associated with a trend toward an increased incidence of serious adverse events (Thadani et al., 1991), a process described by Waters (1991) as proischemia. Although bradycardia, transient asystole, and exacerbation of heart
failure have been reported with verapamil, these responses usually have
occurred after intravenous administration of verapamil, in patients with
disease of the SA node or AV nodal conduction disturbances, or in the
presence of A novel Ca2+ channel blocker, mibefradil, is an example of an agent that inhibits both the T- and L-type Ca2+ channels. The T-type Ca2+ channel contributes to the spontaneous contractile function of smooth muscle cells (Mishra and Hermsmeyer, 1994). Mibefradil was demonstrated to be effective in reducing the frequency and duration of asymptomatic ischemic episodes in patients with stable exertional angina pectoris and asymptomatic ischemia (Braun et al., 1996) and received approval from the United States Food and Drug Administration (FDA) for use as an antianginal agent. However, it subsequently was withdrawn from the market due to adverse drug interactions, possibly due to its dual inhibition of both the P-glycoprotein and CYP3A systems (Wandel et al., 2000). Recent observational studies and a metaanalysis have raised concerns about the long-term safety of the Ca2+ channel blockers, and in particular, short-acting nifedipine preparations (Psaty et al., 1995; Pahor et al., 1995; Furberg et al., 1995). Authors of a recent analysis based on a total of 100 clinical studies of Ca2+ channel blockers concluded that observational studies and randomized clinical trials give concordant evidence linking adverse safety effects to short-acting Ca2+ channel blockers, specifically to short-acting nifedipine (Opie et al., 2000). The proposed hypothesis for this adverse effect lies in abrupt vasodilation with reflex sympathetic activation. A similar conclusion was reached by Stason et al. (1999), who performed a systematic review of the literature on nifedipine and determined that adverse effects were observed in patients on monotherapy with an immediate-release formulation of nifedipine. Therapeutic Uses Variant Angina Variant angina is a direct result of a reduction in flow, not the result of an increase in oxygen demand. Controlled clinical trials have demonstrated efficacy of the Ca2+ channel blocking agents for the treatment of variant angina (Antman et al., 1980; Severi et al., 1980). These drugs can attenuate ergonovine-induced vasospasm in patients with variant angina, which suggests that protection in variant angina is due to coronary dilation rather than to alterations in peripheral hemodynamics (Waters et al., 1981). Exertional Angina Ca2+ channel antagonists also are effective in the treatment of exertional, or exercise-induced, angina. The utility of these agents may result from an increase in blood flow due to coronary arterial dilation, from a decrease in myocardial oxygen demand (secondary to a decrease in arterial blood pressure, heart rate, or contractility), or from both. Numerous double-blind placebo-controlled studies have shown that these drugs decrease the number of anginal attacks and attenuate exercise-induced depression of the ST segment. The 'double product,' which is calculated as heart rate x systolic blood pressure, is an indirect measure of myocardial oxygen demand. Since these agents reduce the level of the double product (or oxygen demand) at a given external work load, and the value of the double product at peak exercise is not altered, the beneficial effect of Ca2+ channel blockers likely is due primarily to a decrease in oxygen demand rather than to an increase in coronary flow. As described above, Ca2+ channel antagonists, particularly
the dihydropyridines, may aggravate anginal symptoms in some patients when
used without a Unstable Angina Medical therapy for unstable angina involves the administration of aspirin,
which reduces mortality, and nitrates, Myocardial Infarction There is no evidence that Ca2+ channel antagonists are of
benefit in the early treatment or secondary prevention of acute myocardial
infarction, and in several trials, the short-acting formulation of the dihydropyridine
nifedipine appears to have had a detrimental effect on mortality at higher
doses (Kloner, 1995; Opie and Messerli, 1995; Yusuf, 1995; Furberg et al.,
1995). Diltiazem and verapamil may reduce the incidence of reinfarction in
patients with a first non-Q-wave infarction who are not candidates for a Other Uses The use of Ca2+ channel antagonists as antiarrhythmic agents is discussed in Chapter 35: Antiarrhythmic Drugs, and their use for the treatment of hypertension is discussed in Chapter 33: Antihypertensive Agents and the Drug Therapy of Hypertension. Clinical trials are under way to evaluate the capacity of Ca2+ channel blockers to slow the progression of renal failure and to protect the transplanted kidney. Verapamil has been demonstrated to improve left ventricular outflow obstruction and symptoms in patients with hypertrophic cardiomyopathy. Verapamil also has been used in the prophylaxis of migraine headaches. While several studies suggest that dihydropyridines may suppress the progression of mild atherosclerosis, there is no evidence that this alters mortality or reduces the incidence of ischemic events. Nimodipine has been approved for use in patients with neurological deficits secondary to cerebral vasospasm after the rupture of a congenital intracranial aneurysm. Nifedipine, diltiazem, and felodipine have been shown to provide symptomatic relief in Raynaud's disease. Ca2+ channel antagonists cause relaxation of the myometrium
in vitro and markedly inhibit the amplitude of spontaneous and oxytocin-induced
contractions. Clinical studies have shown Ca2+ channel blockers to
be effective in stopping preterm uterine contractions (Murray et al.,
1992; Childress and Katz, 1994; Evidence Report/Technology Assessment, 2000).
In studies comparing nifedipine with the |
![]() -Adrenergic
Receptor Antagonists
-Adrenergic
Receptor Antagonists
|
The Therapeutic Uses Unstable Angina
Myocardial Infarction
|
Comparison of Antianginal Therapeutic Strategies
|
In evaluating trials in which different forms of antianginal therapy are compared, careful attention must be paid to the patient population studied, including the pathophysiology and stage of the disease. It also is important to realize that an important placebo effect may be seen in these trials. The efficacy of antianginal treatment will depend on the severity of angina, on the presence of coronary vasospasm, and on the factors underlying myocardial oxygen demand. It also is most helpful if the dose of each agent is titrated to maximum benefit. Considering the precipitants of angina in a given patient often is
helpful. In patients with normal left ventricular function who have
predictable angina with exertion despite nitrate therapy, Combination Therapy Since the different categories of antianginal agents utilize different mechanisms of action, it has been suggested that combinations of these agents would allow the use of lower doses, increasing effectiveness and reducing the incidence of side effects. However, despite the potential advantages, combination therapy in practice rarely fully achieves this potential and may be accompanied by serious side effects. Nitrates and The concurrent use of organic nitrates and Ca2+ Channel Blockers and When angina is not adequately controlled by nitrates and a Fluctuations in coronary tone long have been recognized as primary in variant angina. It also is likely that increased tone superimposed on fixed disease plays a role in the variable anginal threshold seen in many patients with otherwise chronic stable angina and possibly in ischemic episodes precipitated by cold and by emotion (Zeiher et al., 1991). Increased coronary tone also may be important in the anginal episodes occurring early after myocardial infarction (Bertrand et al., 1982) and after coronary angioplasty, and it probably accounts for those patients with unstable angina who respond to dihydropyridines (Hugenholtz et al., 1981). Atherosclerotic arteries have abnormal vasomotor responses to a number of stimuli (Kaplinsky, 1992; Oemar et al., 1998), including exercise, other forms of sympathetic activation, and cholinergic agonists; in such vessels, stenotic segments actually may become more severely stenosed during exertion. This implies that the normal exercise-induced increase in coronary flow is lost in atherosclerosis. Similar exaggerated vascular contractile responses are seen in hyperlipidemia, even before anatomic evidence of atherosclerosis develops. Because of this, coronary vasodilators (nitrates and/or Ca2+ channel blockers) are an important part of the therapeutic program in the majority of patients with ischemic heart disease. Ca2+ Channel Blockers and Nitrates In severe exertional or vasospastic angina, the combination of a nitrate and a Ca2+ channel blocker may provide additional relief over that obtained with either type of agent alone. Since nitrates primarily reduce preload, whereas Ca2+ channel blockers reduce afterload, the net effect on reduction of oxygen demand should be additive. However, excessive vasodilation and hypotension can occur. The concurrent administration of a nitrate and nifedipine has been advocated in particular for patients with exertional angina with heart failure, the sick-sinus syndrome, or AV nodal conduction disturbances, but excessive tachycardia may be seen. Ca2+ Channel Blockers, In patients with exertional angina that is not controlled by the
administration of two types of antianginal agents, the use of all three may
provide improvement, although the incidence of side effects increases
significantly (Tolins et al., 1984; Asirvatham et al., 1998).
The dihydropyridines and nitrates dilate epicardial coronary arteries; the
dihydropyridines decrease afterload; the nitrates decrease preload; and the |
Antiplatelet and Antithrombotic Agents
|
Unlike other antianginal agents, aspirin clearly has been demonstrated to reduce mortality in patients with unstable angina, reducing the incidence of myocardial infarction and death. In addition, low doses of aspirin appear to reduce the incidence of myocardial infarction in patients with chronic stable angina, and aspirin, given in doses of 160 to 325 mg at the onset of treatment of myocardial infarction, clearly reduces mortality, presumably by inhibiting the increased platelet aggregation that accompanies thrombolytic therapy (Kerins and FitzGerald, 1991). Heparin, in its unfractionated form and as low-molecular-weight heparin, also has been shown to reduce angina and prevent infarction in unstable angina. More direct thrombin inhibitors, such as hirudin, which directly inhibit even clot-bound thrombin, are not affected by circulating inhibitors, and function independently of antithrombin III, are being investigated. A metaanalysis of the GUSTO-IIB, TIMI-9B, OASIS-1, and OASIS-2 trials showed that in patients with acute myocardial ischemia without ST segment elevation there was a modest reduction in the risk of death or myocardial infarction at 35 days when hirudin was compared with unfractionated heparin, but an increase in bleeding, with the majority of the benefit occurring in patients not receiving thrombolytic agents (OASIS-2 Investigators, 1999). Further studies seem warranted. Thrombolytic agents, on the other hand, have been shown to be of no benefit in unstable angina (Anonymous, 1992). Intravenous inhibitors of the platelet glycoprotein IIb/IIIa receptor (abciximab, tirofiban, and eptifibatide) have proven to be effective in preventing the complications of percutaneous coronary interventions and in the treatment of patients presenting with acute coronary syndromes (Bhatt and Topol, 2000). In contrast, orally active platelet glycoprotein IIb/IIIa antagonists have not proven to be effective in the chronic treatment of patients with ischemic heart disease and may result in worse outcomes. It is possible that there are subsets of patients with unstable angina who have different response profiles. |
Prospectus
|
It is anticipated that new therapeutic agents in ischemic heart disease will fall into two categories. The first will include agents that modify cellular actions via cell surface or intracellular receptors but have no effect on gene expression. The second will include agents that either permanently or transiently alter gene expression, either by enhancing or inhibiting the production of a normal cell product, or by rendering the cell capable of producing an entirely new product. This gene-based therapy (see Chapter 5: Gene Therapy) will assume increasing importance in the treatment of ischemic heart disease. Emerging agents in the nitrate category include molsidomine, a nitrate-like agent that appears to produce vascular smooth muscle relaxation utilizing mechanisms similar to those of the nitrates themselves. A number of Ca2+ channel antagonists are under development
in the classes of dihydropyridines (nitrendipine), phenylalkylamines (gallopamil,
a verapamil derivative), and piperazines (flunarizine, which is
marketed in some countries outside the K+ channel activators, such as cromakalim, pinacidil,
and nicorandil, have been proposed for use as direct coronary
vasodilators in the treatment of both vasospastic and chronic stable angina (Hamilton
and Weston, 1989; Why and Richardson, 1993; Lablanche et al., 1993).
Studies of nicorandil (Kukovetz et al., 1992) demonstrate that
its relaxant effect on coronary arterioles is inhibited by the K+
channel blocker, glyburide, and thus is likely due to K+ channel
activation, with attendant cellular hyperpolarization of vascular smooth
muscle. However, this agent also exerts a nitrate-like effect, stimulating
guanylyl cyclase to increase cyclic GMP, primarily in epicardial coronary
arteries, including stenotic segments. The relative importance of these
separate effects in human beings is not known. In studies of relatively small
sample size, nicorandil had antianginal efficacy similar to that of nitrates;
the Angiotensin converting enzyme (ACE) inhibitors (see Chapters 31, 33, and 34) are useful not only in the treatment of hypertension but also in reducing morbidity and mortality in symptomatic and asymptomatic congestive heart failure (Cohn et al., 1986; CONSENSUS Trial Study Group, 1987; Pitt, 1994). It also has been suggested that these agents may have a beneficial effect in angina pectoris over and above their effects on blood pressure, but it has been difficult to demonstrate this effect in normotensive patients. In addition to the ability of these agents to reduce blood pressure, which would be expected to have a favorable effect on ventricular wall stress, they also may reduce the coronary vascular response to angiotensin II and may prevent deleterious ventricular remodeling. Lisinopril has been suggested to reduce mortality when used in the treatment of acute infarction in the GISSI-III trial. However, if coronary perfusion pressure is lowered, ACE inhibitors have the potential to have a deleterious effect on angina; this may account for the patients who have become worse with these drugs in some trials (Vogt et al., 1993). In the HOPE trial, the ACE inhibitor rampiril resulted in a reduction in myocardial infarction and death from cardiovascular causes in patients with vascular disease or with diabetes plus one other cardiovascular risk factor, but without conventional indications for the use of an ACE inhibitor (Yusuf et al., 2000). Our appreciation of the role of inflammation in the development and progression of atherosclerosis and of unstable coronary syndromes is evolving (Libby, 2000; Ridker et al., 2000). Clinical studies are in progress that will address the ability of antibiotics, antiinflammatory agents, and HMG-CoA reductase inhibitors to retard the atherosclerotic process and reduce cardiac events. There has been great interest in evaluating the therapeutic utility of angiogenic factors, stem cells, and endothelial progenitor cells to facilitate growth of new vessels in areas of ischemia (Asahara et al., 2000; Isner, 2000; Kalka et al., 2000). Promising results have been achieved using vascular endothelial growth factor (VEGF) and related agents in human patients (Schumacher et al., 1998; Hendel et al., 2000). Several problems in the treatment of myocardial ischemia lend themselves to the use of gene-based therapies. Because coronary angioplasty is so commonly followed by restenosis (30% to 40% of cases) and because conventional pharmacological therapy has not abolished this problem, the concept of altering the biology of the cellular response to angioplasty has emerged. Techniques for delivering vectors to localized segments of peripheral and coronary vessels and vein grafts have been developed, and functional genes have been transferred (Chapman et al., 1992; Lemarchand et al., 1993; Nabel, 1995; Duckers and Nabel, 2000; O'Blenes et al., 2000). In animal models, the tendency for restenosis has been significantly inhibited (Ohno et al., 1994), and clinical trials are planned. Building on the success with angiogenic factors mentioned above, studies with animals have demonstrated that transferring the gene coding for VEGF also is efficacious (Isner, 2000), and trials in human beings are under way. In an attack on one mechanism underlying the development of atherosclerosis, it recently has been shown that retroviral therapy restores apo-E levels in apo-E deficient mice and reduces the extent of atherosclerosis (Hasty et al., 1999). Alternatively, disruption of the 12/15-lipoxygenase gene also was protective in this mouse model, consistent with a role for inflammation in the atherosclerotic process (Cyrus et al., 1999). These areas of rapid progress suggest that therapy with genotypic strategies will play a significant role in the future. For further discussion of acute myocardial infarction and ischemic
heart disease see Chapters 228 and 226 in Harrison's Principles of
Internal Medicine, 16th ed., |
|
Politica de confidentialitate | Termeni si conditii de utilizare |

Vizualizari: 1235
Importanta: ![]()
Termeni si conditii de utilizare | Contact
© SCRIGROUP 2024 . All rights reserved